[dropcap]Z incemia means the zinc level in blood plasma is too low to meet metabolic needs of the body for this mineral.
Q: How important is a normal blood level of zinc?
A: A low blood level of zinc is characterized by widespread alterations in energy metabolism, growth, hemoglobin, carbon dioxide transport, hormone activity, insulin storage, many enzyme activities, prostaglandin function, collagen production, male fertility, protein synthesis, and vitamin A metabolism.
What Is Zincemia In Celiac Disease and/or Gluten Sensitivity?
Testing Thigh Strength. Courtesy Charlie Goldberg, M.D., UCSD School of Medicine
What Is Hypophosphatemia?
[dropcap]H ypophosphatemia means the level of phosphates in the bloodstream is too low to meet metabolic needs of the body for this mineral.
Q: How important is phosphorus in metabolism?
A: Phosphorus is crucial to life, being present in every cell of the body and constitutes 45% of skeletal bone weight along with 40% calcium needed to support the body as a framework.
A low blood phosphate level is characterized by alterations in blood acid-alkaline balance and serious neuromuscular, hematologic, renal, skeletal, and dental abnormalities.
Symptoms result primarily from decreased production of adenosine triphosphate (ATP), the main energy source in cells, and phosphocreatine, a secondary energy source for muscle contraction.
Acute phosphorus deficiency may precipitate rhabdomyolysis which is destruction of muscle.
Nervous system dysfunction is observed in severe hypophosphatemia.
Chronic phosphorus deficiency causes proximal myopathy (upper arms and thighs).1
Severe phosphorus deficiency has widespread and ultimately fatal consequences.
What Is Hypophosphatemia In Celiac Disease and/or Gluten Sensitivity?
Sources:
Takeda E, Ikeda S, Nakahashi O. Lack of phosphorus intake and nutrition. Clin Calcium. 2012 Oct;22(10):1487-91. [↩]
What Is Plummer-Vinson Syndrome Affecting the Esophagus?
[dropcap]P[/dropcap]lummer-Vinson syndrome is a manifestation of severe, long-term, iron deficiency anemia that is characterized by post-cricoid esophageal webs and dysphagia.
Q: What are esophageal webs?
A: Esophageal webs are one or more thin horizontal membranes consisting of squamous epithelium (cells that line the surface of the esophagus) and submucosa. They usually protrude from the anterior (front) wall, extending laterally across the inside esophagus but not to the posterior (rear) wall, which means that they rarely encircle the lumen.1
Dysphagia, or difficulty swallowing, from these webs is commonly painless and intermittent or progressive and may cause obstruction.
Webs can be detected by barium swallow X-ray, but the best way for demonstration is videofluoroscopy and by upper gastrointestinal endoscopy. They appear smooth, thin, and gray with eccentric or central lumen space. The webs typically occur in the upper part of the esophagus and may be missed and accidentally ruptured unless the endoscope is introduced under direct visualization.1
Iron deficiency is believed to decrease the contraction amplitude or force of the esophageal muscle resulting in motility impairment. Slower transit times have been recorded at the proximal and middle parts of the esophagus of Plummer-Vinson syndrome patients compared to healthy volunteers.2 Transit time is how fast ingested food and fluids travel through the esophagus.
Gude et al, report that iron replacement does not necessarily reverse the dysphagia in all the cases of Plummer-Vinson syndrome and that close monitoring of the web is mandated to watch for malignant change. In fact, 3 to 15 per cent of the patients with Plummer-Vinson syndrome, mostly women between 15 and 50 years of age, have been reported to develop esophageal or pharyngeal cancer.2
What Is Plummer-Vinson Syndrome Affecting the Esophagus In Celiac Disease and/or Gluten Sensitivity?
Sources:
Novacek G. Plummer-Vinson syndrome. Orphanet J Rare Dis. 2006; 1: 36. Published online 2006 September 15. doi: 10.1186/1750-1172-1-36. [↩] [↩]
Gude D, Bansal DP, and Malu A. Revisiting Plummer Vinson Syndrome. Annals of Medical and Health Sciences Research. 2013 Jan-Mar;3(1):119-121. [↩] [↩]
[dropcap]A utoimmune disorders refer to those conditions that involve an abnormal attack on the body’s own tissues perpetuated by the production of autoantibodies directed against self.
Q: What happens when autoantibodies attack the body’s own tissues?
A: This abnormal immune activity by autoantibodies causes inflammation and damage to targeted body tissues.
Dermatitis herpetiformis is a skin manifestation of celiac disease characterized by extremely itchy blisters that commonly erupt on forearms and knees but may appear on the face, scalp or buttocks.
Autoimmune diseases as a group affect approximately 8.5% of people worldwide.
What Are Autoimmune Disorders In Dermatitis Herpetiformis?
Figure on right shows how atherosclerosis impedes blood flow through coronary arteries while blood clots block blood flow. Courtesy Google.
What Is Coronary Artery Disease (CAD)?
[dropcap]C[/dropcap]oronary artery disease (CAD), also called ischemic heart disease, is a gradual narrowing of medium and large arteries of the heart by fatty buildups, called atherosclerotic plaques.
It is characterized by slowly developing interference with blood flow to heart tissue itself, resulting in oppressive chest pain called angina and, ultimately, thrombosis (clot) causing heart attack.
The heart is a muscular organ that is working all the time, so it needs a constant supply of oxygen. Oxygen is brought to the working heart tissue by the coronary arteries with each beat of the heart. When heart muscle has to work harder, it needs more oxygen delivered to itself. Lack of oxygen causes pain.
In fact, failure of diseased coronary arteries to deliver adequate oxygen to heart tissue is the most common cause of angina pectoris – substernal pain (under breastbone) or pressure brought on by exertion and relieved by rest.
Thrombosis, or clot formation, occurs when blood cells within a narrowed artery can no longer get through. Trapped, blood cells pile up and block the artery thus triggering a cascade of events called heart attack. Coronary arteries that are narrowed by atherosclerotic plaques can rupture causing injury to the coronary blood vessel resulting in blood clotting which blocks the flow of blood to the heart muscle. Blood clots may form, partially dissolve, and later form again and angina can occur each time a clot blocks blood flow in an artery.1
Q: How does coronary artery disease develop?
A:Coronary artery disease slowly develops from this combination of events:
Dysfunction of epithelial cells that line the inside of arteries cause the vessels to stiffen, and subsequently
Accumulation of lipid (fat) in smooth muscle cells beneath the inside lining of arteries and in foam cells cause buildup of fatty deposits on the inside walls progressing to fibrous plaque formation.
Oxidized low-density lipoprotein (oxLDL), so-called bad cholesterol, and oxysterols play important roles in the development of atherosclerosis. OxLDL triggers the immune system to produce autoantibodies against oxLDL that are detectable in serum. These antibodies are called anti-oxLDL. Anti-oxLDL antibody and oxysterol concentrations are associated with coronary artery stenosis. Oxidative stress may be greatly increased in unstable angina.2 and Chronic inflammation in the general population is a major risk factor for ischemic heart disease.
The pathophysiology of atherosclerosis is, clearly, different in women when compared to the men. The women have a higher risk of blood coagulability making them at high risk for the blood clot formation. In a large number of women endothelial dysfunction, small vessel size and diffuse atherosclerosis have been identified as causes of ischemia without evidence of blockade in the coronary arteries.3
Also, atherosclerotic plaque in women is less fibrotic and contains more lipid filled foam cells, implying greater potential for reversibility but also potentially greater vulnerability for plaque rupture and thrombosis.4
Who is Affected in the General Population?
Coronary artery disease remains the leading cause of death in developed countries despite significant progress in primary prevention and treatment strategies.
It is the leading cause of death in women, as well as an important cause of disability.
Older patients are at particularly high risk of poor outcomes following acute coronary syndrome.5
What Is Coronary Artery Disease In Celiac Disease and/or Gluten Sensitivity?
Ischemic heart disease is the leading cause of death in the United States, making cardiovascular risk assessments and potential interventions or treatments imperative for patients with celiac disease.6
Yasunobu Y, Hayashi K, Shingu T, Yamagata T, Kajiyama G, Kambe M. Coronary atherosclerosis and oxidative stress as reflected by autoantibodies against oxidized low-density lipoprotein and oxysterosis. Atherosclerosis. Apr 2001;155(2):445-53. [↩]
Kunadian V, Ford GA, Bawamia B, Qiu W, Manson JE. Vitamin D deficiency and coronary artery disease: A review of the evidence. Am Heart J. 2014 Mar;167(3):283-291. doi: 10.1016/j.ahj.2013.11.012. Epub 2013 Dec 19. [↩]
Kunadian V, Ford GA, Bawamia B, Qiu W, Manson JE. Vitamin D deficiency and coronary artery disease: A review of the evidence. Am Heart J. 2014 Mar;167(3):283-291. doi: 10.1016/j.ahj.2013.11.012. Epub 2013 Dec 19. [↩]
Kunadian V, Ford GA, Bawamia B, Qiu W, Manson JE. Vitamin D deficiency and coronary artery disease: A review of the evidence. Am Heart J. 2014 Mar;167(3):283-291. doi: 10.1016/j.ahj.2013.11.012. [↩]
Robinson BL, Davis SC, Vess J, Lebel, J. Primary care management of celiac disease. Nurse Practitioner. February 2015: Vol 40 – Issue 2; 28–34. [↩]
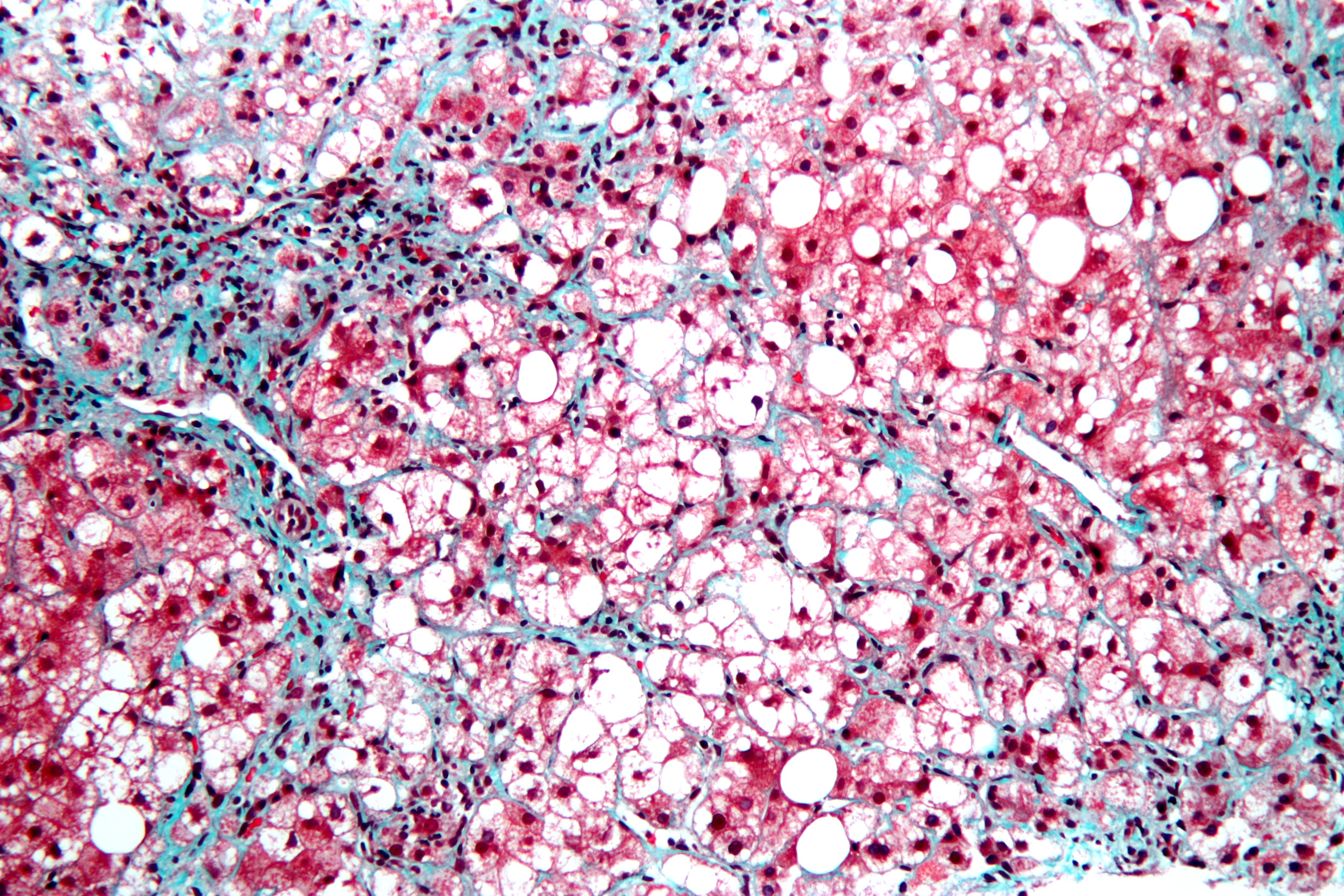
This is a stained liver biopsy sample showing advanced cellular changes in non-alcoholic fatty liver disease. Blue is fibrosis. White is fat accumulation in degenerated cells. Courtesy of Nephron’s work.
What Is Non-Alcoholic Fatty Liver Disease?
[dropcap]N on-alcoholic fatty liver is a non-inflammatory liver disorder characterized by degenerative changes in the liver caused by excessive accumulation of lipid (fat) in hepatocytes (liver cells) that is called free fatty acid-generated lipotoxicity.
Non-alcoholic fatty liver shows an increase in liver enzymes called transaminases.
Q: What are the enzymes that increase?
A: The transaminases that increase are ALT and AST. ALT is the abbreviation for alanine aminotransferase enzyme and AST is the abbreviation for aspartate aminotransferase enzyme. They are commonly measured in blood tests to determine liver function and when elevated indicate inflammation.
What Is Non-Alcoholic Fatty Liver In Celiac Disease and/or Gluten Sensitivity?
What Is Intraepithelial Lymphocytosis In Normal Small Bowel Samples? [dropcap]I ntraepithelial lymphocytosis is characterized by an abnormal increase in the numbers of intraepithelial lymphocytes (IELs) that are present in the small intestinal mucosa. Q: What…
[dropcap]M uscle pain and tenderness, also called myalgia, is a disorder of muscle tissue.
Muscle pain that is ongoing or chronic can result from a variety of disorders, infections, overuse, injury, as an unwanted effect of certain medications, toxic substances, celiac disease, and certain nutritional deficiencies.
What Is Muscle Pain and Tenderness In Celiac Disease and/or Gluten Sensitivity?
[dropcap]E rythema nodosum is an inflammatory disorder involving the deep dermis layer of skin and subcutaneous fat septa that underlies the skin. It is characterized by eruptions of recurrent or persistent multiple painful, red nodules under the skin that leave a bruised appearance when healing and do not scar.
The lower legs are most affected, but sores can appear anywhere there is subcutaneous fat.
Q: How do the nodules develop in erythema nodosum?
A: The edges of nodules are poorly defined, and the nodules vary from 2-6 cm.
During the first week of eruption, nodules become tense, hard, and painful. During the second week, they change color from bright red to bluish or livid and may become soft, but do not ulcerate. As absorption progresses, the color gradually fades to a yellowish hue, resembling a bruise. This disappears in 1 or 2 weeks as the overlying skin sloughs off and is replaced.1
The eruptive phase of erythema nodosum begins with flulike symptoms of fever and generalized aching followed by a painful rash within 1-2 days. Aching legs and swelling ankles may occur and precede the eruption or appear during the eruptive phase and may persist for weeks.2
Currently, the most common cause of erythema nodosum is streptococcal infection in children and streptococcal infection and sarcoidosis in adults.3Most sores in infection-induced erythema nodosum heal within 7 weeks, but active disease may last up to 18 weeks.
In contrast, 30% of idiopathic erythema nodosum cases may last more than 6 months. Idiopathic means that the cause is not known.
What Is Erythema Nodosum In Celiac Disease and/or Gluten Sensitivity?
 What Is Zincemia?
What Is Zincemia?






![Crohnie_sores_4[1]](https://glutenfreeworks.com/health/wp-content/uploads/sites/10/Crohnie_sores_41.jpg)