[dropcap]U[/dropcap]nexplained weight gain is characterized by increased body mass due to excess fat accumulation that is not desired by the individual.
A body mass index (BMI) of 25 to 30 signifies being overweight.
What Is Unexplained Weight Gain In Celiac Disease and/or Gluten Sensitivity?
Malnourished Infant With Acute Diarrhea and Swollen Belly.
What Is Acute Diarrhea?
[dropcap]A cute diarrhea is a small intestinal motility disorder characterized by excessively rapid movement of intestinal contents through the small intestine with excessive loss of fluid and electrolytes that leads rapidly to a life threatening hypokalemia (low potassium blood level) and acidosis.
Q: What is hypokalemia?
A: Hypokalemia is characterized by dehydration that may result in vascular collapse, muscular malfunction that may result in paralytic ileus (bowels do not move), paralysis (cannot stand), and respiratory hypoventilation (shallow breathing) or failure, metabolic acidosis resulting from diarrhea, and impaired nerve conduction.1
While diarrhea may be a common symptom of small bowel mucosal disease, the consequent malabsorption can lead to substantial malnutrition and nutrient deficiencies. The small intestine, unlike the colon, has been relatively inaccessible, and systematic evaluation is often necessary to identify and treat small intestinal mucosal diseases that lead to diarrhea. All patients with severe diarrhea or diarrhea associated with features suggestive of malabsorption may have a disease of the small intestinal mucosa that requires careful evaluation and targeted management.2
What Is Acute Diarrhea In Celiac Disease and/or Gluten Sensitivity?
Murray JA1, Rubio-Tapia A. Diarrhoea due to small bowel diseases. Best Pract Res Clin Gastroenterol. 2012 Oct;26(5):581-600. doi: 10.1016/j.bpg.2012.11.013. [↩]
What Are Erosions In The Second Part Of The Duodenum?
[dropcap]E rosions in the second part of the duodenum typically are superficial excoriations (sores) in the mucosal lining that do not penetrate into the muscle layer as does an ulcer.
Of note, most erosions develop in the first part of the duodenum rather than the second part.
Q: Are duodenal erosions serious?
A: Yes duodenal erosions are serious and can be life-threatening for the following reasons:
Duodenal erosions may occur together with gastric erosions, therefore they can jointly induce massive bleeding.
Duodenal erosions may be associated with duodenal ulcer but hemorrhage originates from the erosion and the ulcer itself does not bleed.
Duodenal erosion in itself might induce bleeding. The intensity of bleeding, if there is no hemorrhage from other places, is not so severe, as the one originating from gastric erosions.1
What Are Erosions In The Second Part Of The Duodenum In Celiac Disease and/or Gluten Sensitivity?
Sources:
Preisich P, Farkas I, Konyár EJ. The role of duodenal erosions in the occurrence of upper gastrointestinal haemorrhage. Scand J Gastroenterol Suppl. 1989;167:36-8. [↩]
Intestinal Edema of Duodenum in an 11 Month Old Baby. Courtesy: Nature.com
What Is Small Intestinal Edema?
[dropcap]S mall intestinal edema is characterized by fluid accumulation within the intestinal mucosa so that the intestinal wall appears thick and swollen.
Intestinal edema hampers peristalsis that can result in pain and gas build-up. Peristalsis is the normal rhythmic muscular wave-like action that moves residue along the gastrointestinal tract.
Q: What part of the small intestinal lining is swollen?
A: Any part of the small intestine may be affected. Some causes of edema include allergic reactions, enteropathies such as celiac disease, cow milk enteropthy, yeast infection, parasite infection, inflammatory bowel disease such as Crohn’s disease, and certain medications.
For example, the anti-hypertensive drugs known as Angiotension Converting Enzyme (ACE) inhibitors can cause intestinal angioedema and therefore the patient may present with gastrointestinal complaints.1
What Is Small Intestinal Edema In Celiac Disease and/or Gluten Sensitivity?
Sources:
LoCascio E J, Mahler S A, and Arnold TC. Intestinal Angioedema Misdiagnosed as Recurrent Episodes of Gastroenteritis. West J Emerg Med. Sep 2010; 11(4): 391–394. [↩]
Underarm showing skin darkening, which is a feature of Addison’s Disease
What Is Primary Addison’s Disease?
[dropcap]A[/dropcap]ddison’s disease is an autoimmune destruction of the adrenal glands by autoantibodies that target the adrenal cortex, or outer part of these glands, and is characterized by a slow progressive failure of the adrenal glands to adequately produce its steroid hormones.
Symptoms of adrenal fatigue or failure may not develop until the majority of adrenal tissue is destroyed. When untreated, progression leads to coma, called Addisonian crisis, which is a medical emergency.
There are two adrenal glands each located on top of a kidney and enclosed in a connective tissue capsule. Each is a small, triangular shape that is made of two parts: the outer region and the inner region.
The inner region, called the adrenal medulla, produces epinephrine and norepinephrine chemicals that are needed to deal with stress.
The outer region, called the adrenal cortex, produces adrenocortical (steroid) hormones and releases them into the bloodstream in response to pituitary stimulating hormone from the brain.
Q: What is the function of steroid hormones produced by the adrenal glands?
A: Functions of the three steroid hormones produced by the adrenal glands are:
Glucocorticoids restrain inflammation and metabolism of carbohydrates, fats and proteins to maintain a normal glucose blood level. The major glucocorticoid is hydrocortisone.
Mineralocorticoids regulate the retention and excretion of fluids and electrolytes by the kidneys. The most important mineralocorticoid is aldosterone.
Androgen (testosterone) is a male sex hormone.
Secondary adrenal insufficiency may develop from other causes that are not immune related such as chronic infections, tumor, and medications.
What Is Addison’s Disease In Celiac Disease and/or Gluten Sensitivity?
[dropcap]A therosclerosis is a disease of arteries involving the buildup of fatty material called plaque along the walls of medium and large arteries characterized by patchy subintimal thickening, hardening, and loss of elasticity of blood vessels.
The intima is the innermost layer of an artery, having contact with blood. The subintima is beneath it.
Q: What happens when arteries become narrowed and less flexible?
A: Narrowing of the inside diameter of blood vessels and hardening of their walls reduce or obstruct blood flow through them which impairs their ability to supply tissues of the body with oxygen and nourishment.
When tissues are deprived of oxygen, pain and dysfunction results such as angina pectoris involving heart muscle because the heart continually needs oxygen never being able to rest.
It is thought that atherosclerosis develops from 1) epithelial cell dysfunction of the intima, and 2) lipid (fat) accumulation in smooth muscle cells and in foam cells, causing buildup of fatty deposits on the inside walls progressing to fibrous plaque formation. That is, intimal smooth muscle cells are surrounded by connective tissue and intracellular and extracellular lipids (fat build-up inside and outside of these cells).
What Is Atherosclerosis In Celiac Disease and/or Gluten Sensitivity?
Microscopic Slide of Biopsy Sample Showing Lymphocytic Colitis. Courtesy Quizlet.com
What Is Lymphocytic Colitis?
[dropcap]L[/dropcap]ymphocytic colitis is a microscopic inflammation of the large intestinal mucosa with infiltration of lymphocytes (IELs) that is characterized by non-bloody secretory diarrhea.
Secretory diarrhea describes bowel movements that consist of a large volume of liquid stool.
Q: What are IELs?
A: IELs is an abbreviation for intraepithelial lymphocytes, which are white blood cells that infiltrate within epithelial cells or between them. Epithelial cells form the surface mucosa of the large intestine also called the colon.
The histopathological criteria (biopsy) for lymphocytic colitis are a density of at least 20 IELs per 100 surface epithelial cells; chronic inflammatory infiltrate of mononuclear cells in the lamina propria; epithelial damage; and a subepithelial collagen layer of less than 10 µm. The increased collagen band consists basically of collagen type I and III, which are the subtypes produced by repair functions, indicating a reactive origin.1That is, the mucosa is reacting to some irritative substance.
Up to 10% of adults undergoing colonoscopy for investigation of chronic diarrhea and having visibily normal appearing mucosa may have lymphocytic colitis.2
Bile acid malabsorption has been shown to coexist in 60% of patients with lymphocytic colitis.1
Lymphocytic colitis (LC) is categorized as primary or secondary. Primary LC is a clinical and histopathological disease of unknown cause. Secondary LC may develop as the result of iritating factors acting on the colon such as smoking or many medications. In one study, the most common drug treatments as a percentage of the study group were corticosteroids (32.1%), proton pump inhibitors (26.0%), antidepressant drugs, specifically selective serotonin reuptake inhibitors (21.4%), angiotensin-converting enzyme inhibitors or angiotensin II receptor antagonists (18.3%), statins (17.6%), thyroid hormones (17.6%), and beta-blockers (16.0%).3
Secondary lymphocytic colitis is associated with several concomitant diseases including celiac disease. This is why lymphocytic changes must be interpreted with caution before considering them as a separate entity of autoimmune origin, instead of secondary reactions to ischemia and toxic stimulants. Efforts must be made to better classify and diagnose patients with real, primary lymphocytic colitis to avoid over-prescription of corticosteroids for treatment.3
What Is Lymphocytic Colitis In Celiac Disease and/or Gluten Sensitivity?
Sources:
Ohlsson B. New insights and challenges in microscopic colitis. Therap Adv Gastroenterol. 2015 Jan;8(1):37-47. doi: 10.1177/1756283X14550134. [↩] [↩]
Abdo AA, Urbanski SJ, Beck PL. Lymphotcytic and collagenous colitis: the emerging entity of microscopic colitis. An update on pathophysiology, diagnosis and management. Canadian Journal of Gastroenterology. Jul 2003;17(7):425-32. [↩]
Roth B, Manjer J, Ohlsson B. Drug Target Insights. 2013 Aug 11;7:19-25. doi: 10.4137/DTI.S12109. [↩] [↩]
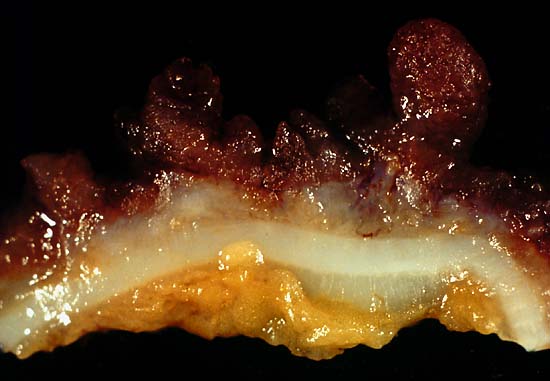
This photo is from a total colectomy done for severe, intractable chronic ulcerative colitis. It shows a close view of a lengthwise section through the colon wall. This demonstrates not only the angry red mucosa, but also, the tendency for the inflamed tissue to throw itself up into inflammatory pseudopolyps. Source: Ed Uthman, MD. Public domain.
What Is Ulcerative Colitis?
[dropcap]U[/dropcap]lcerative colitis is an inflammatory disorder of the colon characterized by continuous inflammation of the mucosa and submucosa usually with small ulcers, extending from the rectum and typically involving the distal colon, rectum, and anus and producing bloody diarrhea.
While the severity of ulcerative colitis varies among patients, iron deficiency anemia often develops due to blood loss especially when there are many bloody bowel movements in a day.
The onset of ulcerative colitis is most commonly in young adulhood.
Q: Is this disease painful?
A: Yes with the passage of stool.
Psychological stress and subsequent dysbiosis exacerbate ulcerative colitis.
Psychological stress activates multiple physiological processes aimed at maintaining balance within the body. These physiological processes also have the capacity to influence the composition of microbial communities in the digestive tract, and research now indicates that exposure to stressful stimuli leads to gut microbiota dysbiosis.1
While the relative abundance of many different bacterial types can be altered during stressor exposure, findings in nonhuman primates and laboratory rodents, as well as humans, indicate that bacteria in the genus Lactobacillus are consistently reduced in the gut during stress.2
Presently, ulcerative colitis cannot be cured. This condition has a course of remissions, when symptoms subside, and flares, when symtpoms get worse. Treatment is aimed to reduce flares and promote remission. In all cases, correction of dysbiosis improves the condition.
Ulcerative colitis is associated with increased incidence of cancer of the colon.3
What Is Ulcerative Colitis In Celiac Disease and/or Gluten Sensitivity?
Sources:
Galley JD, Bailey MT. Impact of stressor exposure on the interplay between commensal microbiota and host inflammation. Gut Microbes. 2014 May 1;5(3):390-396. Epub 2014 Apr 1. [↩]
Galley JD, Bailey MT. Impact of stressor exposure on the interplay between commensal microbiota and host inflammation. Gut Microbes. 2014 May 1;5(3):390-396. Epub 2014 Apr 1. [↩]
Taber’s Cyclopedic Medical Dictionary. F. A. Davis. Philadelphia, PA [↩]
[dropcap]A[/dropcap]ortic vasculitis is an inflammatory disease of the aorta that causes dilation of the aorta wall with narrowing of the inside passageway and results in widespread impairment of blood flow to tissues served by the aorta.
Q: What is the result of inflammatory disease of the aorta?
A: The aorta is the largest artery in the body. It extends from the left ventricle (lower chamber) of the heart and carries blood out of the heart with each beat to rest of the body. Narrowing of the aorta’s inside diameter due to swelling from inflammation causes elevated blood pressure and enlarged heart because of back pressure of blood unable to be fully pumped out of the heart with each beat. The heart enlarges because the difficulty of pumping blood out makes it work harder than normal.
Vasculitis that causes midaortic syndrome is a variety of aortic coarctation (narrowing) located in the lower thoracic aorta, the abdominal aorta or both, involving the intestinal and renal vessels (kidney). It usually presents with arterial hypertension.1
What Is Aortic Vasculitis In Celiac Disease and/or Gluten Sensitivity?
Sources:
Massel D. n-3 polyunsaturated fatty acids reduced mortality and morbidity after recent myocardial infarction. Therapeutics. Jan-Feb 2000:6 [↩]
Microscopic Image Showing a Pink Collagen Band in Collagenous Colitis.
What Is Collagenous Colitis?
[dropcap]C[/dropcap]ollagenous colitis is a disease of the large intestine (colon) that is characterized by microscopic inflammation of the surface mucosal lining and an abnormally thickened collagen band of tissue that develops wthin the lining of the colon.
The thicker than normal layer of collagen of at least 10 µm (reference value: 2–7 µm) can vary in different locations. Inflammation occurs with increased numbers of lymphocytes (white blood cells) and plasma cells and epithelial (surface cell) damage. These changes can only be seen under microscopic examination of multiple biopsied tissue samples taken during a colonoscopy procedure.
Q: What is collagen?
A:Collagen is a strong, fibrous protein found in connective tissue of the colon and many other tissues such as tendons. The normal basement membrane in the bowel consists mainly of collagen type IV, laminin, and fibronectin. The increased collagen band observed in collagenous colitis consists basically of collagen type I and III, which are the subtypes produced by repair functions, indicating a reactive origin to some irritant or drug.1
The biopsies should preferably be taken from the ascending colon, since the pathological hallmarks may be absent in the descending colon, and in the normally occurring thicker collagen layer in the rectosigmoid region.1 Inflammation of the ileum (last segment of the small intestine next to colon) is common.2
Endoscopy and radiological (x-ray) examinations are usually normal.3
Autoimmune disorders are frequently seen in adult patients with collagenous colitis.4 In the study below by Koskela et al. concomittent autoimmune diseases were present in 53% of patients with collagenous colitis.5
Importantly, the finding of collagenous colitis in patients with autoimmune diseases may reflect the treatment with NSAIDs (non-steroidal anti-inflammatory drugs), such as Ibuprofin and aspirin, PPIs (proton pump inhibitors), and other drugs. However, if secondary forms of collagenous colitis are not taken into consideration, underlying, treatable diseases may be overlooked, while only the gastrointestinal symptoms are treated symptomatically or with budesonide (a steroid).6
Treatment with budesonide steroid is efficacious irrespective of bile acid malabsorption.7
Budesonide at a mean dose of 4.5 mg/day maintained clinical remission for at least 1 year in the majority of patients with collagenous colitis and preserved health-related quality of life without safety concerns. Treatment extension with low-dose budesonide beyond 1 year may be beneficial given the high relapse rate after budesonide discontinuation.8
See below for nutritional deficiency problems caused by steroid usage and steps to be taken for correction.
What Is Collagenous Colitis In Celiac Disease and/or Gluten Sensitivity?
Sources:
Ohlsson B. New insights and challenges in microscopic colitis. Therap Adv Gastroenterol. 2015 Jan;8(1):37-47. doi: 10.1177/1756283X14550134. [↩] [↩]
Bjørnbak C, Engel PJ, Nielsen PL, Munck LK. Microscopic colitis: clinical findings, topography and persistence of histopathological subgroups. Aliment Pharmacol Ther. 2011 Nov;34(10):1225-34. doi: 10.1111/j.1365-2036.2011.04865.x. [↩]
Abdo AA, Urbanski SJ, Beck PL. Lymphotcytic and collagenous colitis: the emerging entity of microscopic colitis. An update on pathophysiology, diagnosis and management. Canadian Journal of Gastroenterology. Jul 2003;17(7):425-32. [↩]
Leung ST, Chandan VS, Murray JA, Wu TT. Collagenous gastritis: histopathologic features and association with other gastrointestinal diseases. Am J Surg Pathol. 2009 May;33(5):788-98. doi: 10.1097/PAS.0b013e318196a67f. [↩]
Koskela RM, Niemela SE, Karttunen TJ, Lehtola JK. Clinical characteristics of collagenous and lymphocytic colitis. Scandanavian Journal of Gastroenterology. Sep 2004;39(9):837-45. [↩]
Ohlsson B. New insights and challenges in microscopic colitis. Therap Adv Gastroenterol. 2015 Jan;8(1):37-47. doi: 10.1177/1756283X14550134. [↩]
Bjørnbak C, Engel PJ, Nielsen PL, Munck LK. Microscopic colitis: clinical findings, topography and persistence of histopathological subgroups. Aliment Pharmacol Ther. 2011 Nov;34(10):1225-34. doi: 10.1111/j.1365-2036.2011.04865.x. [↩]
Münch A, Bohr J, Miehlke S, et al. Low-dose budesonide for maintenance of clinical remission in collagenous colitis: a randomised, placebo-controlled, 12-month trial. Gut. 2014 Nov 25. pii: gutjnl-2014-308363. doi: 10.1136/gutjnl-2014-308363. [↩]
![Obesity_001_[1]](https://glutenfreeworks.com/health/wp-content/uploads/sites/10/Obesity_001_1.jpg)