Source: Ed Uthman, MD. Public domain.
Contents
What Is Ulcerative Colitis?
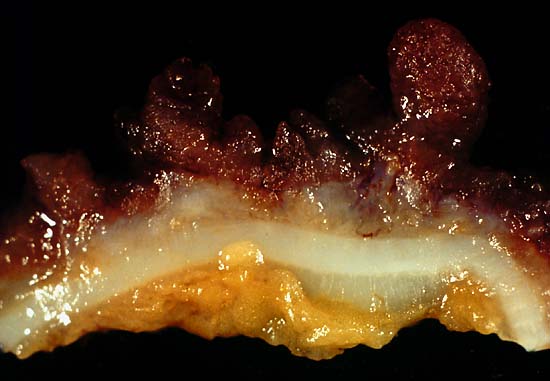
[dropcap]U[/dropcap]lcerative colitis is an inflammatory disorder of the colon characterized by continuous inflammation of the mucosa and submucosa usually with small ulcers, extending from the rectum and typically involving the distal colon, rectum, and anus and producing bloody diarrhea.
While the severity of ulcerative colitis varies among patients, iron deficiency anemia often develops due to blood loss especially when there are many bloody bowel movements in a day.
The onset of ulcerative colitis is most commonly in young adulhood.
Q: Is this disease painful?
A: Yes with the passage of stool.
Psychological stress and subsequent dysbiosis exacerbate ulcerative colitis.
Psychological stress activates multiple physiological processes aimed at maintaining balance within the body. These physiological processes also have the capacity to influence the composition of microbial communities in the digestive tract, and research now indicates that exposure to stressful stimuli leads to gut microbiota dysbiosis.1
While the relative abundance of many different bacterial types can be altered during stressor exposure, findings in nonhuman primates and laboratory rodents, as well as humans, indicate that bacteria in the genus Lactobacillus are consistently reduced in the gut during stress.2
Presently, ulcerative colitis cannot be cured. This condition has a course of remissions, when symptoms subside, and flares, when symtpoms get worse. Treatment is aimed to reduce flares and promote remission. In all cases, correction of dysbiosis improves the condition.
Ulcerative colitis is associated with increased incidence of cancer of the colon.3
What Is Ulcerative Colitis In Celiac Disease and/or Gluten Sensitivity?
-
This Is A Normal Cecum (Area Between Small And Large Intestine) For Comparison. Relationship between ulcerative colitis and celiac disease. Ulcerative colitis is an associated inflammatory disorder of celiac disease.
-
Relationship between ulcerative colitis and diagnosis. Diagnosis can be challenging because abdominal pain, diarrhea, and associated iron deficiency anemia develop in ulcerative colitis and these symptoms are some of the many features of celiac disease.
-
Relationship between ulcerative colitis and type of disease. Study patients with ulcerative colitis and celiac disease were found more likely to have severe colitis but not aggressive disease and had a trend toward greater use of immunomodulators.4
- Relationship between ulcerative colitis and non-response to gluten free diet in person with celiac disease. Celiac disease patients with persistent gastrointestinal symptoms despite a gluten free diet should trigger evaluation for underlying ulcerative coilitis.5
How Prevalent Is Ulcerative Colitis In Celiac Disease and/or Gluten Sensitivity?
- There is significantly increased prevalence (7%) of familial ulcerative colitis in patients with celiac disease.6
- In the group of 80 ulcerative colitis patients, coexistence of celiac disease basing on serological histopatological investigation was found in 4 patients (5%).7
What Are The Symptoms Of Ulcerative Colitis?
Ulcerative colitis is marked by these symptoms:
- Rectal bleeding.
- Frequent diarrhea with outpouring of blood, mucous, and pus increasing fecal content.
- Pain with the passage of stool.
- Probable weight loss, anemia from blood loss, and nutritional deficits.
How Does Ulcerative Colitis In Celiac Disease and/or Gluten Sensitivity Develop?
- Ulcerative colitis results from unclear mechanism that involves disrupted homeostatic interactions between the microbiota and the mucosal immune system as a result of multiple genetic and environmental factors.
- Ulcerative colitis is exacerbated by pschological stress.
- Vitamin A and omega-3 fatty acid deficiencies may exacerbate ulcerative colitis.8
Does Ulcerative Colitis Respond To Gluten-Free Diet?
Gluten free diet prevents increased disease from malnutrition and malignancy in untreated celiac disease.
In a cross sectional study of patients with inflammatory bowel disease, a diagnosis of celiac disease was reported by 10 (0.6%) respondents and 81 (4.9%) respondents reported non-celiac gluten sensitivity. Three hundred fourteen (19.1%) participants reported having previously tried a gluten free diet and 135 (8.2%) reported current use of gluten free diet. Overall 65.6% of all patients, who attempted a gluten free diet, described an improvement of their gastrointestinal symptoms and 38.3% reported fewer or less severe IBD flares. In patients currently attempting a gluten free diet, excellent adherence was associated with significant improvement of fatigue.9
Note: Caraway is particularly helpful to reduce inflammation and improve healing of ulcerative colitis. Please see below under Carminatives, Step #6.
LOW RESIDUE DIET that is gluten free is the diet of choice for ulcerative colitis to reduce inflammation and promote healing. Fiber allowed is 10 to 15 grams a day.
Here we are talking about fiber in plants and the need to eat reduced soluble fiber and to avoid insoluble fiber.
Soluble fiber. Soluble means it dissolves in water, which is the major component of digestive juices. This fiber promotes movement of contents through the digestive tract and feeds the billions of normal, essential microbes that inhabit the gut, which are necessary for colon health. (Please view Dysbiosis post.) Monitor the amount of soluble fiber you eat because too much can cause diarrhea.
On the other hand, in ulcerative colitis, it is important to avoid insoluble fiber, meaning it does NOT dissolve in water. Because it is indigestible, this fiber causes greatly increased fermentation by normal microbe populations in the colon and results in gas build-up which stretches the bowel wall and produces pain, acidity which harms the mucosa setting the stage for ulcerations, and bulkiness of stool which hurts the colon wall and makes defecation more difficult in this condition. Actually, this fiber rapidly expands to 4 times it’s bulk within the stomach.
Insoluble fiber is naturally found in the bran layer of grains, seeds and nuts and the skins of fruits, seeds of berries, legumes, and vegetables. Avoid dried fruits, figs, berries, nuts, seeds and popcorn. Grocery store products that have nutritional labels such as crackers and baked goods often have added these insoluble fiber ingredients: guar gum, dextrin, cellulose, carrageen, polydextrose or resistant starches.
6 Steps To Improve Ulcerative Colitis In Celiac Disease and/or Gluten Sensitivity:
- [dropcap]1[/dropcap]Remove the Trigger. Maintain a Strict, Nutritious Gluten Free Diet:
[box type=”shadow” ]Treatment. This condition responds to the complete elimination of gluten, which is the required treatment that improves both ulcerative colitis and gut health.
- Gut health is the foundation to restore ALL health. Restored health will enable you to maintain a strict gluten free diet, just as other life tasks will be easier.
- A strict gluten free diet means removing 100% of wheat, barley, rye and oats from the diet.
- Cutting out bread and other obvious sources of gluten is not good enough for recovery. Even 1/8th teaspoon of flour or bread crumb is enough to sustain the inflammation that is damaging your small intestine, causing increased permeability (leaky gut) and allowing undigested gluten to enter your body where it can damage structures and function, and instigate immune inflammatory responses.
Correct Your Individual Nutritional Needs.
- Eat foods that can replenish missing nutrients. Find them under NUTRIENT DEFICIENCIES.
- Take nutritional supplements as needed. Find them under NUTRIENT DEFICIENCIES.
Recovery from gluten sensitivity. You should begin to feel better within a week and notice more energy as inflammation subsides and the absorbing cells that make up the surface lining of your small intestine are better able to function.
- Intestinal lining cells are replaced every 5 days. The healing process is like sunburn where the damaged surface layer of skin sloughs off and is replaced with new normal cells.
- Leaky gut normally resolves in two month after starting a gluten free diet and brings about a big improvement in health. Improvement in intestinal permeability precedes morphometric recovery (cell appearance and structure) of the small intestine in celiac disease.10
- The intestinal lining may take up to a year to heal.[/box]
- [dropcap]2[/dropcap] Reduce Inflammation. Foods to Eat and Foods Not to Eat:
Because gluten is inflammatory, eliminate OTHER inflammatory foods from your diet to reduce an additive effect to gluten. At the same time, try to eat foods that reduce inflammation (anti-inflammatory).
[box type=”shadow” ]Here Are Major Inflammatory Food Types That Reduce Healing:
- Damaging Foods. In susceptible persons, includes corn, dairy (cow), and soy. Lactose, the sugar in any animal milk disrupts intestinal permeability causing leaky gut.11
- Allergenic Foods. Includes foods that trigger the immune sytem to produce IgE antibodies. Allergy testing is the usual way to discover these offending foods.
- Shelf Stable Processed Foods. Includes any that contain additives and preservatives. Look for them on the nutrition label of the box or package. Additives and preservatives also disrupt intestinal permeability causing leaky gut.11
- Fats. Limit deep fried foods, trans-fats, saturated fats (animal fat/butter), and EXCESSIVE omega-6 fatty acid oils like corn oil. Rancid fats, sodium caprate (a medium chain fat), and sucrose monester fatty acid (a food grade surfactant) induce significant disruption of the intestinal barrier that causes leaky gut.11.
- Excessive Refined White Flours. Includes products made from them such as cookies, bread, cakes, pies. Bran contains the vitamins and minerals that metabolize grains and slows the otherwise rapid entry of sugar from their digestion into the bloodstream. Also disrupt intestinal permeability causing leaky gut.11
- Refined Sugars. Includes white sugar, corn fructose and high fructose corn syrup.
- Certain Spices. Includes paprika and cayenne pepper which disrupt intestinal permeability causing leaky gut.11
- Alcohol and Caffeine. Disrupt intestinal permeability causing leaky gut.11[/box]
[box type=”shadow” ]Here Are Important Anti-Inflammatory Food Types to Promote Health:
- Fruits. Contain ample amounts of vitamins, minerals and phytochemicals which are naturally occuring components in plants that detoxify toxins, carcinogens (reducing the risk by 50%) and mutagens. In ulcerative colitis, avoid dried fruits.
- Non-Starchy Vegetables. Support intestinal integrity and provide ample amounts of vitamins, minerals and phytochemicals. Includes green leafy vegetables such as lettuce and well cooked kale, also onion, broccoli, garlic, and others as tolerated.
- High Quality Complex Carbohydrates. Provide vitamins, minerals, and fiber while boosting serotonin levels to help you relax and feel calm. Includes well cooked root vegetables such as carrots, parsnips, sweet potatoes, turnips, red beets, and others.
- Antioxidants. Protect the body from inflammatory oxidant molecules that continually occur and help us handle stress and reduce irritability. Includes vitamin C-containing foods such as lemon, grapefruit, apricot, Brussels sprouts and strawberries, and others. Also, includes vitamin E-containing foods such as avocado. Cocoa is good, too. Avoid seeds but use their oils, especially olive oil, canola oil, and sunflower oil (unless allergic).
- Omega-3 Fatty Acids. Balance opposing omega-6 fatty acids and bad fats. Fish sources includes tuna, salmon, cod, and others. Plants sources include canola oil, purslane, and others. Note: In this condition, flax and chia seeds should be avoided because of their indigestible fiber BUT their oil is very good to improve health.
- Probiotics. Supply normal microbes needed for colon health and health of the body such as these fermented foods: yogurt, kefir, and unpasteurized apple cider or rice vinegar.
- Prebiotics. Food with soluble fiber as found in fruits and veggies keeps our population of colonic microbes healthy, BUT in ulcerative colitis undigestible fiber (insoluble fiber) such as that found in the bran coating of seeds, whole grains and whole nuts should be avoided because this fiber is rough and causes large stools that are harmful.
- Protective Herbs and Spices. See below #6 for examples, especially caraway.[/box]
- [dropcap]3[/dropcap] Information Sheet You Can Take to Your Doctor or Other Health Professional:
Click here.
- [dropcap]4[/dropcap] Manage Your Medications Safely:
[box type=”shadow” ]
Certain medications deplete vitamin A which may exacerbate ulcerative colitis. Ask your doctor or pharmacist about this possible adverse effect if you are taking any of the drugs listed below. Do not stop prescribed medications without supervision.
This is not a complete listing.
ANTACIDS / ULCER MEDICATIONS
- Pepcid®, Tagamet®, Zantac® deplete Vitamin A.
- Magnesium and Aluminum Antacid preparations (Gaviscon®, Maalox®, Mylanta®) deplete Vitamin A.
CHOLESTEROL DRUGS
- Colestid® and Questran® deplete Vitamin A.
WEIGHT LOSS DRUGS THAT BIND FAT also interfere with absorption of some nutrients.
- Zenicol (Orlistat®) depletes Vitamin A.
[/box]
- [dropcap]5[/dropcap]Nutritional Supplements To Help Correct Deficiencies:
[box type=”shadow” ]
The type and quantity of nutritional supplements that may be needed depend on which nutrients are deficient.
- Multivitamin/mineral combination once a day is useful to improve overall nutrient levels. This is a safe dose, but always check with your doctor to avoid interactions with medications.
- Vitamin A as prescribed following blood test for status.
Storage Note: Store container tightly sealed, away from heat, moisture and direct light to avoid loss of potency. That is, in a safe kitchen cabinet – not in the bathroom or on the kitchen table.[/box]
- [dropcap]6[/dropcap]Manage Natural Remedies:
[box type=”shadow” ]Hydration:
- Eight glasses of water are recommended per day unless there is a contraindication such as kidney or heart disease. The Institute of Medicine recommends approximately 2.7 liters (91 ounces) of total water, from all beverages and foods, each day for women and 3.7 liters (125 ounces) daily of total water for men.
- If you are thirsty, drink water. Add fresh, squeezed lemon to water. Lemon is anti-inflammatory, alkalizing and provides vitamin C.
- Hydration Test: Urine should be pale yellow. Fingertips should be plump, without pruning but this may not be reliable when fingers are swollen with edema. Lips should be plump, without puckering. The feeling of thirst can be unreliable.
- What is wrong with soda, coffee, tea, and alcohol? These drinks are dehydrating, increase acid, and deplete nutrients.[/box]
[box type=”shadow” ]Carminatives. The following anti-inflammatory plant sources called carminitives help heal the digestive tract. They also tone the digestive muscles which improves peristalsis, thus aiding in the expulsion of gas from the stomach and intestine to relieve digestive colic and gastric discomfort.
Carminative Food Remedies:
- Raspberry.
- Carrot is also a cleansing digestive tonic.
- Grape is also bile stimulating and a cleansing remedy for sluggish digestion and laxative.
- Redbeets also stimulate and improve digestion and are easily digested.
- Cabbage also stimulates and improves digestion and is also a liver decongestant.
- Lettuce also stimulates and improves digestion and is also an alterative, meaning it improves the function of organs involved with the digestion and excretion of waste products to bring about a gradual change.
- Potatoes are antispasmodic (due to atropine like properties) and a liver remedy.
Carminative Herb Remedies:
- Caraway, in addition to being carminative, is particularly helpful in healing the gut mucosa including severe inflammation and ulcerations, having these properties: anti-inflammatory, anti-spasm, antimicrobial, antioxidant, and immunomodulatory (ability to modify or regulate immune functions).12
- Sage is also a digestive, astringent, bile stimulant and energy tonic that heals the mucosa. Drink as tea or use in cooking.
- Chamomile, lemon balm, and fennel, (as a tea) also help relieve nervous tension.
- Parsley also relieves indigestion.
- Rosemary as a tea and in cooking also is a nervous system tonic for stress and fatigue, bile stimulant, and can relieve headaches and indigestion.
- Thyme is also soothing remedy useful for stimulating digestion of rich, fatty foods.
Carminative Spice Remedies:
- Cloves are also antispasmodic.
- Nutmeg is also useful for indigestion.
- Ginger.[/box]
[box type=”shadow” ]Exercise Helps: Exercise improves circulation and rids the body of toxins.
- Walking is aerobic exercise that reconditions the whole body to improve stamina. Read more about Exercise and Fitness.
- Weight training builds muscle. Read more about Exercise and Fitness.
- Stretching improves flexibilty. Read more about Exercise and Fitness.
Note: Exercise is important, but the amount and type of exercise undertaken depends on your health. Your first priority is to heal. [/box]
What Do Medical Research Studies Tell About Ulcerative Colitis?
RESEARCH STUDY SUMMARIES
“Prevalence of a gluten-free diet and improvement of clinical symptoms in patients with inflammatory bowel diseases.” This cross-sectional study investigating the widespread acceptance in the United States of maintaining a gluten-free diet without an underlying diagnosis of celiac disease found that in a large group of patients with inflammatory bowel disease (IBD), a substantial number had attempted a gluten free diet, of whom the majority had some form of improvement in gastrointestinal symptoms. Testing a gluten free diet in clinical practice in patients with significant intestinal symptoms, which are not solely explained by the degree of intestinal inflammation, has the potential to be a safe and highly efficient therapeutic approach.
A gluten free diet questionnaire was used in 1647 patients with inflammatory bowel diseases participating in the CCFA Partners longitudinal Internet-based cohort.
RESULTS: A diagnosis of celiac disease was reported by 10 (0.6%) respondents and 81 (4.9%) respondents reported non-celiac gluten sensitivity. Three hundred fourteen (19.1%) participants reported having previously tried a gluten free diet and 135 (8.2%) reported current use of gluten free diet. Overall 65.6% of all patients, who attempted a gluten free diet, described an improvement of their gastrointestinal symptoms and 38.3% reported fewer or less severe IBD flares. In patients currently attempting a gluten free diet, excellent adherence was associated with significant improvement of fatigue (P < 0.03).9
“Impact of coexistent celiac disease on phenotype and natural history of inflammatory bowel diseases.” This case-control study investigating the frequency of co-occurrence of celiac disease and inflammatory bowel disease in comparison with other autoimmune disorders found that patients with ulcerative colitis and celiac disease were more likely to have severe colitis and had a trend toward greater use of immunomodulators.
Study was performed at two hospital referral centers. Cases comprised of patients with known diagnoses of celiac disease and inflammatory bowel disease (IBD). Two random IBD controls without celiac disease were selected for each case after matching for IBD type. Disease phenotype and natural history for both Crohn’s disease (CD) and ulcerative colitis (UC) were noted from medical record review, and were compared between IBD patients with and without celiac disease.
Identified were a total of 51 patients with IBD (22 UC, 1 indeterminate colitis, 28 CD) and celiac disease. There was no significant difference in the age, gender, or ethnicity between celiac-IBD and controls. Pancolitis (severe colitis) was more common in celiac-UC patients as compared with controls. There was also a trend toward increased use of immunomodulators among celiac-UC patients than in non-celiac UC controls. There were no significant differences in IBD-related medication usage, hospitalizations, or surgeries.5
“Effects of Carum carvi L. (Caraway) extract and essential oil on TNBS-induced colitis in rats.” This study investigating the effects of caraway extract (CHE) and its essential oil (CEO) in an immunological model of severe colitis in rats demonstrated data suggesting that caraway fractions are both effective and possess anti-colitic activity irrespective of the dose and route of administration. This study confirms that caraway, a common herb, is beneficial for inflammatory bowel disease.
Tissue damage induced by TNBS manifested severe inflammation, hemorrhage, ulcer, and necrosis as well as thickening of colon wall in colitis control groups. TNBS model of experimental colitis is beneficial for the screening of drugs with anticolitic activity and has several similarities to pathological and clinical features of the human ulcerative colitis.
Different doses of CHE (100, 200, 400 mg/kg) and CEO (100, 200, 400 μl/kg) were administered orally and also doses of CHE (100, 400 mg/kg) and CEO (100, 400 μl/kg) were given intraperitoneally to the 6 separate groups of male Wistar rats. Administration of the doses started 6 h after induction of colitis and continued daily for 5 consecutive days. Wet colon weight/length ratio was measured and tissue damage scores as well as indices of colitis were evaluated both macroscopically and histopathologically. CHE and CEO at all doses tested were effective in reducing colon tissue lesions and colitis indices and the efficacy was nearly the same when different doses of plant fractions were administered. Administration of the steroids prednisolone (4 mg/kg by mouth), Asacol® (mesalazine microgranules 100 mg/kg) and hydrocortisone acetate 20 mg/kg intraperitoneally as references were effective in reducing colon tissue injures as well.12
“Celiac disease and other autoimmunological disorders coexistence.” This study investigating the occurrence of other autoimmune disorders associated with celiac disease found that coexistence of coeliac disease with other autoimmune diseases is quite frequent. In the group of 110 patients with diagnosed gluten enteropathy the coexistence of autoimmune disease, such as diabetes mellitus type 1 in 7.2% cases, hyperthyreosis on 1.8% of cases, vitiligo in 0.9% of cases, primary biliary cirrhosis in 2% of cases and rheumatoidal arthritis in 0,9 of cases.
In the group of 80 ulcerative colitis patients, coexistence of celiac disease basing on serological histopatological investigation was found in 4 patients (5%).7
“Familial occurrence of inflammatory bowel disease in celiac disease.” This case control study evaluating the familial occurrence of inflammatory bowel disease (IBD) in 600 first degree relatives of 111 consecutive patients with celiac disease revealed 10 cases of IBD of whom 7 cases were ulcerative colitis and 3 cases were Crohn’s disease.13
CASE REPORT SUMMARIES
“Ulcerative colitis in a 6-year-old boy with severe celiac disease.” This case report describes a 6-year-old boy with a delay in physical and psychomotor development, rickets, severe anemia and bloody diarrhea. He was diagnosed with celiac disease and ulcerative disease. Ulcerative colitis should be considered in celiac children on restrictive gluten-free diet with persistent diarrhea or bleeding from lower gastrointestinal tract. Screening for celiac disease should be considered in children with ulcerative colitis with impaired physical development and lack of remission despite proper treatment.14
“Co-Occurrence of Celiac Disease and Ulcerative Colitis in a 12-Year-Old Girl.” This case report describes the diagnosis of celiac disease in a 12-year-old girl with ulcerative colitis. The reporting physicians state, “Distinguishing both diseases in one patient could be difficult due to the overlapping symptoms, but it is very important considering completely different therapeutic approaches.”15
“Multiple Disease Associations in Autoimmune Polyglandular Syndrome Type II. “ This case report describes the course of a 25 year old female with a history of ulcerative colitis, celiac disease and type 1 diabetes who presented with mental status changes. She was diagnosed with Hashimoto’s encephalopathy and treated with high dose steroids and intravenous immunoglobulin. She recovered well from her encephalopathy but her post-hospitalization course was complicated due to the development of Addison’s disease, vitiligo, sero-negative arthritis, and hypothyroidism.
This patient had a dramatic development of eight autoimmune diseases over the course of ten years. She developed Addison’s disease, hypothyroidism, type 1 diabetes, Hashimoto’s encephalopathy, vitiligo, celiac disease, sero-negative arthritis, and ulcerative colitis. This represents a particularly aggressive course of APS II and this combination of autoimmune diseases has not been previously reported. It highlights the potential complexity and severity of the clinical course of APS II.16
“Celiac disease in a child with ulcerative colitis: a possible genetic association.” This case report describes finding celiac disease and ulcerative colitis (UC) in an 8-year-old child with a history of anemia and failure to thrive who presented with bloody diarrhea. His evaluation showed anemia, elevated inflammatory markers, and positive celiac antibodies. Endoscopic evaluation revealed partial duodenal villous atrophy and pancolitis. He was diagnosed with celiac disease and UC and responded well to a gluten-free diet and steroid/mesalamine therapy. The patient’s genetic testing revealed markers showing susceptibility for both celiac disease and UC. The reporting physicians state, “It is important to be aware of this association as both conditions can present with similar clinical features, however, require different therapeutic approaches.”17
Sources:- Galley JD, Bailey MT. Impact of stressor exposure on the interplay between commensal microbiota and host inflammation. Gut Microbes. 2014 May 1;5(3):390-396. Epub 2014 Apr 1. [↩]
- Galley JD, Bailey MT. Impact of stressor exposure on the interplay between commensal microbiota and host inflammation. Gut Microbes. 2014 May 1;5(3):390-396. Epub 2014 Apr 1. [↩]
- Taber’s Cyclopedic Medical Dictionary. F. A. Davis. Philadelphia, PA [↩]
- Oxford EC, Nguyen DD, Sauk J, Korzenik JR, Yajnik V, Friedman S, Ananthakrishnan AN. Impact of coexistent celiac disease on phenotype and natural history of inflammatory bowel diseases. Am J Gastroenterol. 2013 Jul;108(7):1123-9. doi: 10.1038/ajg.2013.20. [↩]
- Oxford EC, Nguyen DD, Sauk J, Korzenik JR, Yajnik V, Friedman S, Ananthakrishnan AN. Impact of coexistent celiac disease on phenotype and natural history of inflammatory bowel diseases. Am J Gastroenterol. 2013 Jul;108(7):1123-9. doi: 10.1038/ajg.2013.20. [↩] [↩]
- Cottone M, Marrone C, Casa A, Oliva L, et al. Familial occurrence of inflammatory bowel disease in celiac disease. Inflammatory Bowel Diseases. Sep 2003;9(5):321-3. 101 [↩]
- Zwolińska-Wcisło M, Galicka-Latała D, Rudnicka-Sosin L, Rozpondek P. Coeliac disease and other autoimmunological disorders coexistence. Przegl Lek. 2009;66(7):370-2. [↩] [↩]
- Kathleen Mahan and Sylvia Escott-Stump, ed. Krause’s Food, Nutrition & Diet Therapy, 10th Edition. Philadelphia, PA. USA: W.B. Saunders Company, 2000. [↩]
- Herfarth HH, Martin CF, Sandler RS, Kappelman MD, Long MD. Prevalence of a gluten-free diet and improvement of clinical symptoms in patients with inflammatory bowel diseases. Inflamm Bowel Dis. 2014 Jul;20(7):1194-7. doi: 10.1097/MIB.0000000000000077. [↩] [↩]
- Cummins AG, Thompson FM, Butler RN, et al. Improvement in intestinal permeability precedes morphometric recovery of the small intestine in coeliac disease. Clinical Science. Apr 2001;100(4):379-86. [↩]
- Farhadi A, Banan A, Fields J, Keshavarzian A. Intestinal barrier: an interface between health and disease. Journal of Gastroenterology and Hepatology. 2003;18:479-91. [↩] [↩] [↩] [↩] [↩] [↩]
- Keshavarz A, Minaiyan M, Ghannadi A, Mahzouni P. Effects of Carum carvi L. (Caraway) extract and essential oil on TNBS-induced colitis in rats. Res Pharm Sci. 2013 Jan;8(1):1-8. [↩] [↩]
- Cottone M, Marrone C, Casa A, Oliva L, et al. Familial occurrence of inflammatory bowel disease in celiac disease. Inflammatory Bowel Diseases. Sep 2003;9(5):321-3. [↩]
- Pawłowska-Kamieniak A, Krawiec P, Pac-Kożuchowska E, Mroczkowska-Juchkiewcz A, Kominek K. [Ulcerative colitis in a 6-year-old boy with severe celiac disease. Pol Merkur Lekarski. 2016 Jan;40(235):21-4. [↩]
- Zaja O1, Popović M, Lesar T, Pavić I, Hojsak I. Co-Occurrence of Celiac Disease and Ulcerative Colitis in a 12-Year-Old Girl. Fetal Pediatr Pathol. 2014 Oct 29. [↩]
- Maturu A, Michels A, Draznin B. Multiple Disease Associations in Autoimmune Polyglandular Syndrome Type II. with autoimmune polyglandular syndrome type II (APS II). Endocr Pract. 2014 Aug 22:1-13. [↩]
- Cheng SX, Raizner A, Phatak UP, Cho JH, Pashankar DS. Celiac disease in a child with ulcerative colitis: a possible genetic association. J Clin Gastroenterol. 2013 Feb;47(2):127-9. doi: 10.1097/MCG.0b013e318250e468. [↩]