Candida Albicans Infection

What Is Candida Albicans Infection?
[dropcap]C[/dropcap]andida albicans infection, called candidosis or candidiasis, is an opportunistic invasion of mucous membrane or skin by candida albicans, an endogenous yeast found in 40 to 80% of normal human beings. A former name for this small, budding fungus is monilia albicans.
Opportunistic means that yeast living on mucosal and skin surfaces does not invade (infect) unless these tissues become unhealthy and therefore cannot protect themselves.
Q: How does candida albicans cause infection?
A: Candida albicans lives on the mucosal surfaces and skin in most people without causing infection (colonizes) because of our normal defenses against invasion. In fact, candida albicans is a very effective colonizer of humans. For example, Russell and Lay found that 47% of 1-month-old infants were orally colonized with candida albicans, and 49% were colonized with other fungi.
During growth within the intestinal tract, the organism senses pH (acidity), oxygen, carbon sources, and the presence of surfaces allowing it to optimize gene expression for a particular environment. With these mechanisms for sensing, candida albicans is able to efficiently colonize humans in infancy.1

Lowered host defenses allow yeast already present on mucosal and skin surfaces to take advantage and can grow rapidly, becoming pathogenic (disease producing) so that infection results.
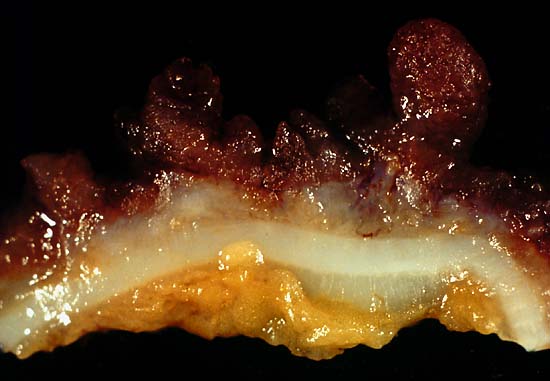
Infection is characterized by superficial, irregular white patches on mucosal surfaces and possible invasion of the bloodstream by a filamentous form (thread-like structures) that can rapidly develop.
Candida albicans is unique among oral pathogens in its ability to invade cornified layers of stratified squamous epithelium of the tongue, mouth surfaces, hard and soft palate, esophagus, and gut. Stratified squamous epithelium is the tough surface cells that ordinarily protect underlying tissues from damage or invasion by microbes.
Candida albicans is also capable of invading the lungs and causing pneumonia and septicemia, which is the spread of infection into the bloodstream.
Here is a time honored simple do-it-youself test for infection of the mouth or throat: First thing in the morning before brushing your teeth or eating, fill a small see through glass with water then gently spit onto the surface. If after an hour the spit remains on the water surface, it is unlikely you have candida in the mouth. If it grows legs downward, it indicates that yeast is growing. If the spit sinks to the bottom, you have this problem. Yeast in the mouth can quickly travel down the esophagus and into the gut.
Medical diagnosis. Difinitive diagnosis for the oral cavity is made by your clinician by swabbing the areas of your mouth and/or throat and viewing under a microscope for evidence of candida.
Infections of the esophagus and gut require inspection by gastroscopy or endoscopy procedure and the taking of samples to be examined under microscope. This examination also give the opportunity to rule out other problems. Barium swallow can show the extent of infection and any disfiguration of the esophagus that results.
What Is Candida Albicans Infection In Celiac Disease and/or Gluten Sensitivity?
Sources:- Rosenbach A, Dignard D, Pierce JV, Whiteway M, Kumamoto CA. Adaptations of Candida albicans for growth in the mammalian intestinal tract. Eukaryot Cell. 2010 Jul;9(7):1075-86. doi: 10.1128/EC.00034-10. Epub 2010 Apr 30. [↩]