Delayed Puberty in Boys
What Is Polymyositis?
[dropcap]P olymyositis is a body-wide connective tissue disease resulting from autoimmune attack of skeletal muscles that is characterized by inflammatory and degeneratory changes. The course is unpredictable being marked by spontaneous flare-ups and remissions.
Polymyositis can begin slowly or abruptly according to the factor that is triggering the onset such as infection, medications like phenytoin, and autoimmune disease.
Progressive muscle weakness starts in the proximal skeletal muscles (muscles closest to the trunk of the body).
Skeletal muscles, also called voluntary, are muscles that move the body as we want, such as walking and lifting objects, as opposed to those we cannot voluntarily control, such as the muscles of digestion.
Q: What are the degeneratory changes in skeletal muscles?
A: In polymyositis, degeneratory changes in skeletal muscles means that muscles are being destroyed (called necrosis), resulting in fibrosis, or scarring. When scar tissue takes the place of lost muscle tissue, it cannot act like muscle to contract and relax. Muscle destruction is what causes muscle pain and weakness.
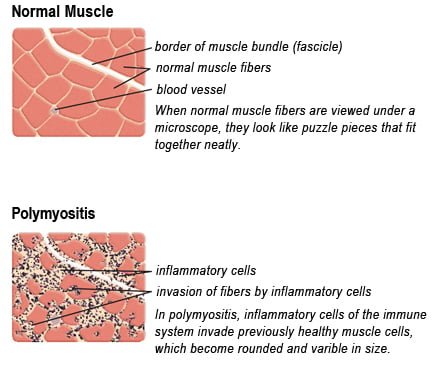
After the clinical work-up of exams and blood studies to determine muscle damage, the diagnosis of polymyositis is confirmed by muscle biopsy. See image at above left. The black dots are inflammatory cells. Edema (fluid) between cells caused by inflammation pushes muscle fibers apart.
There is no cure for polymyositis, but the symptoms can be treated. Options include medication, physical therapy, exercise, heat therapy (including microwave and ultrasound), orthotics and assistive devices, and rest. The standard treatment for polymyositis is a corticosteroid drug, given either in pill form or intravenously. Immunosuppressant drugs, such as azathioprine and methotrexate, may reduce inflammation in people who do not respond well to prednisone.
Periodic treatment using intravenous immunoglobulin can also improve recovery. Other immunosuppressive agents used to treat the inflammation associated with polymyositis include cyclosporine A, cyclophosphamide, and tacrolimus. Physical therapy is usually recommended to prevent muscle atrophy and to regain muscle strength and range of motion.1
Diagnosis is based on elevated muscles enzymes, increased urinary creatine level, and electromyograph abnormalities.
Polymyositis can affect people at any age. It is most common in adults between ages 50 and 70, and in children ages 5 to 15. It affects women twice as often as men and is more common in African Americans than Caucasians.2 The major causes of death from polymyositis are cancer and lung disease, including pneumonia. The 5-year mortality rate can be as high as 1 in 5 patients.2




![Aphthous_ulcer[1]](https://glutenfreeworks.com/health/wp-content/uploads/sites/10/Aphthous_ulcer1.jpg)

