What Is Autoimmune Thyroiditis (Hypothyroidism)?
What Is Autoimmune Thyroiditis (Hypothyroidism)?
[dropcap]A[/dropcap]utoimmune thyroiditis, also called Hashimoto’s thyroiditis or Hashimoto’s Disease, is an autoimmune destruction of thyroid tissue characterized by insufficient thyroid hormone circulating in the body that causes formation of a goiter (enlarged thyroid gland) and hypothyroidism.
Hypothroidism refers to the condition of markedly reduced secretion of thyroid hormone. There are other causes of hypothyroidism besides Hashimoto’s thyroiditis.
Hashimoto’s thyroiditis is often associated with other autoimmune diseases such as celiac disease.
In Hashimoto’s thyroiditis, a profusion of antibodies are produced, which build up in the blood. Left untreated so that much of the thyroid gland is destroyed, this condition may progress to the very serious and life-threatening condition called myxedema.
Note: In myxedema, protein, electrolytes, and water abnormally accumulate in between cells which produce firm, inelastic puffy skin that is cool, dry, rough, scaly, and may appear yellow; in some people, areas such as the ankles become crusty with a look of tree bark. Many systemic changes develop shown by significant slowing of mental and physical functions. Please see below.
Q: What thyroid tissue is targeted for destruction?
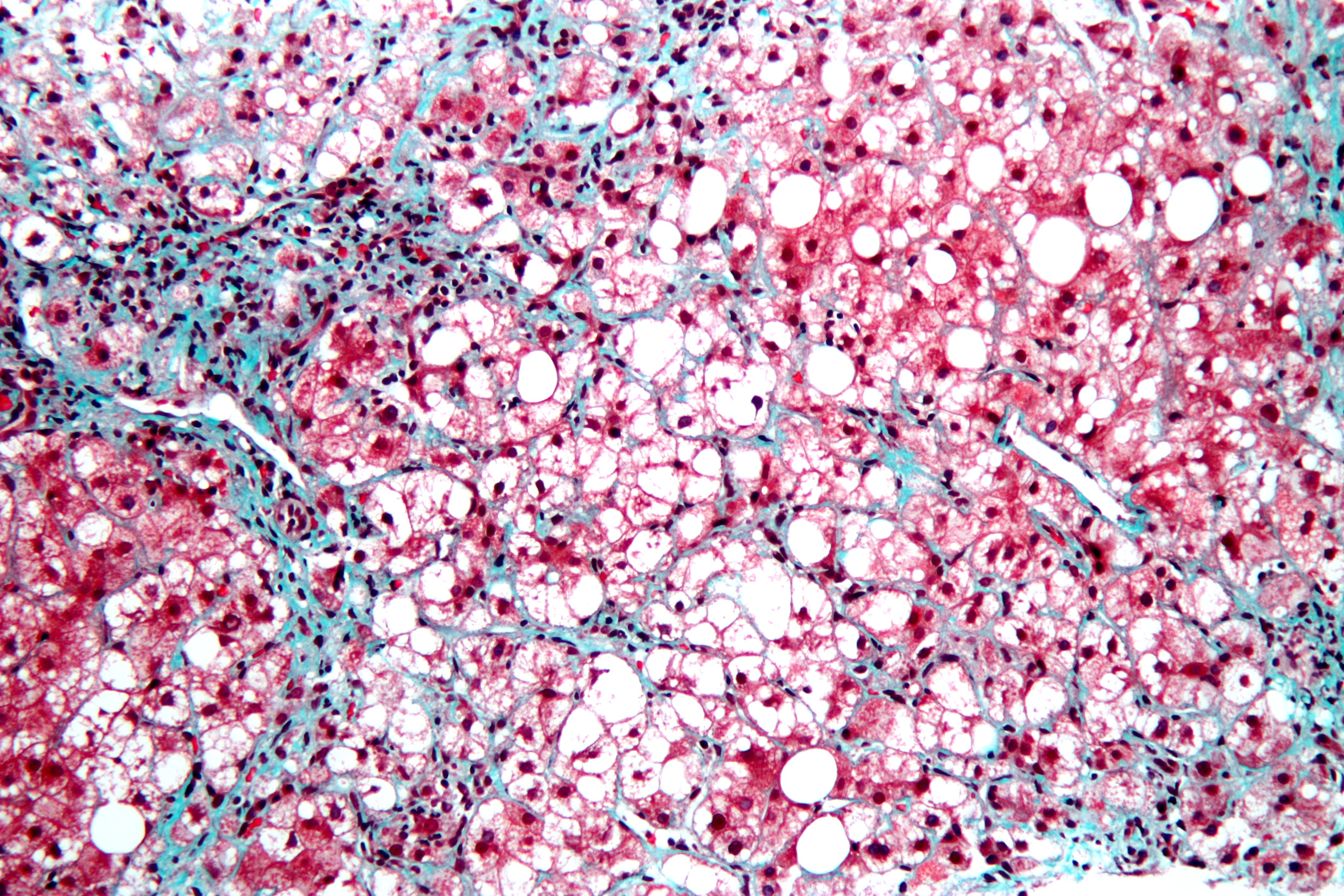
A: In Hashimoto’s thyroiditis, high levels of autoantibodies target thyroglobulin and thyroid peroxidase, leading to inflammation and destruction of the thyroid gland. The resulting fibrosis or scarring of the gland results in lack of thyroid hormone production.
The thyroid gland consists of a large number of closed vesicles that contain a homogenous substance called colloid, which contains the thyroglobulin. Thyroglobulin is an iodine-containing protein secreted by the thyroid gland and stored within its colloid, from which the thyroid hormones thyroxine (T4) and triiodothyroinine (T3) are derived.
T3 is the active hormone and is made from T4. Thyroid hormones affect metabolism, brain development, breathing, heart and nervous system functions, body temperature, muscle strength, skin dryness, menstrual cycles, weight, and cholesterol levels.
Thyroid hormone production is regulated by thyroid-stimulating hormone (TSH), which is made by the pituitary gland in the brain. Normally, when thyroid hormone levels in the blood are low, the pituitary releases more TSH. When thyroid hormone levels are high, the pituitary decreases TSH production.
Hashimoto’s disease, with or without the development of hypothyroidism, is treated with synthetic thyroxine, which is man-made T4. Health care providers prefer to use synthetic T4, such as Synthroid® (Levothyroxine), rather than synthetic T3, because T4 stays in the body longer, ensuring a steady supply of thyroid hormone throughout the day. The thyroid preparations made with animal thyroid are not considered as consistent as synthetic thyroid.
What Is Autoimmune Thyroiditis In Celiac Disease and/or Gluten Sensitivity?
Sources: