[dropcap]E xtraintestinal lymphomas (non-Hodgkin’s) are malignancies that arise in peripheral lymphatic tissue outside the intestinal tract from B-cell and T-cell lymphocytes.
Q: What is peripheral lymphatic tissue?
A: Peripheral lymphatic tissue includes lymph vessels, lymph, lymph nodes, and lymphocytes.
Lymph vessels branch into all the tissues of the body, carrying lymph, a clear fluid that contains white blood cells, especially B-cell and T-cell lymphocytes.
Lymph vessels are connected to lymph nodes which are small, round masses of tissue that store white blood cells. They also trap and remove bacteria or other harmful substances that may be in the lymph. Groups of lymph nodes are found in the neck, underarms, chest, abdomen, and groin.
Ninety percent (90%) of extraintestinal lymphomas are B-cell type and ten percent (10%) are T-cell type. In this malignancy, lymph nodes are replaced by cancer cells. Some are more aggressive than others.
In 2010, there were an estimated 509,065 people living with non-Hodgkin lymphoma in the United States according to the National Cancer Institute.
What Are Extraintestinal Lymphomas In Celiac Disease and/or Gluten Sensitivity?
Malignant lymphoma high grade B-cell. Courtesy Wikimedia
What Is B-Cell Non-Hodgkin’s Lymphoma?
[dropcap]B cell non-Hodgkin’s lymphoma is a malignant, monoclonal (arising from a single cell) proliferation of lymphocytes that is preceded by lymphadenopathy and characterized by varying, less predictable spread than Hodgkin’s disease.
Lymphadenopathy is enlargement of lymph nodes greater than 1.5 cm caused by activation and increased production of lymphocytes and phagocytes (type of white blood cell that engulfs pathogens during infection) or invasion by a tumor.
Q: How does this type of lymphoma develop?
A: 80% to 85% of non-Hodgkin’s lymphoma arise from B-lymphocytes (B-cells).
What Is B Cell Non-Hodgkin’s Lymphoma In Celiac Disease and/or Gluten Sensitivity?
EATL of Jejunum with Thickening And Yellowish Ulcers Visible. Courtesy pubcan.org
What Is Enteropathy-Associated T-Cell Lymphoma?
[dropcap]E nteropathy associated T-cell lymphoma (EATL), although rare, is a tumor of intraepithelial lymphocytes. It is the most common primary gastrointestinal T-cell lymphoma and is characterized by its aggressive course and poor prognosis.
Primary means this malignancy starts out in the intestinal wall rather than spreading to it from a tumor somewhere else in the body.
EATL usually affects the jejunum and grossly (visible to the eye) appears as multiple ulcers causing circumferential thickening of affected bowel wall without the formation of definite tumor masses most commonly in the proximal small bowel. As such, patients may present with intestinal perforation, obstruction or hemorrhage.1
Mesenteric lymph nodes in the abdomen are commonly involved.2
Q: How is EATL diagnosed?
A: Work-up of EATL must include immunohistology, T-cell flow cytometry, T-cell rearrangement and adequate imaging with CT and PET scanning.3
Management of EATL requires a combination of early diagnosis and treatment by surgical resection followed by chemotherapy to achieve treatment success. Overall however, the treatment completion rate remains at 50% and EATL carries a poor prognosis with a 5-year survival rate of <20%.4
What Is Enteropathy-Associated T-Cell Lymphoma In Celiac Disease and/or Gluten Sensitivity?
Sources:
Pun AH, Kasmeridis H, Rieger N, Loganathan A. Enteropathy associated T-cell lymphoma presenting with multiple episodes of small bowel hemorrhage and perforation. J Surg Case Rep. 2014 Mar 20;2014(3). pii: rju013. doi: 10.1093/jscr/rju013. [↩]
Yang DH, Myung SJ, Chang HS, et al. A case of enteropathy-associated T-cell lymphoma presenting with recurrent hematochezia. Korean Journal of Gastroenterology = Taehan Sohwagi Hakhoe Chi. Dec 2003;42(6):527-32. [↩]
Meijer JWR, Mulder CJJ, Goerres MG, Boot H, Schweizer JJ. Coeliac disease and (extra)intestinal T-cell lymphomas: definition, diagnosis and treatment. Scandanavian Journal of Gastroenterology. Dec 2004;39(Suppl 241):78,7p. [↩]
Pun AH, Kasmeridis H, Rieger N, Loganathan Enteropathy associated T-cell lymphoma presenting with multiple episodes of small bowel hemorrhage and perforation.A. J Surg Case Rep. 2014 Mar 20;2014(3). pii: rju013. doi: 10.1093/jscr/rju013. [↩]
Mesenteric Lymph Node Cavitation. Courtesy McBride OM, Skipworth RJ, Leitch D, Yalamarthi S.
What Is Mesenteric Lymph Node Cavitation And Hyposplenism?
[dropcap]M esenteric lymph node cavitation and hyposplenism combination is a rare lymphatic entity. It is characterized by involution (degeneration) of a mesenteric lymph node (abdominal) and absence of functional spleen tissue.
Q: What is happening to the lymph nodes?
A: Lymph nodes are enlarged with central, partly cystic degeneration. When cut open either at surgery or autopsy, milky fluid exudes from the cut surface.
In regards to absent spleen function, the body is highly susceptible to bacterial invasion such as pneumonia because tissues of the spleen, called the pulp, produce specialized white blood cells that protect the body against bacterial invasion and trap foreign antigens.
What Is Mesenteric Lymph Node Cavitation And Hyposplenism In Celiac Disease and/or Gluten Sensitivity?
[dropcap]L ymphadenopathy is an alteration of lymph nodes that is characterized by enlargement of lymph nodes greater than 1.5 cm caused by proliferation (increased production) of lymphocytes within the node.
Q: What are lymph nodes?
A: Lymph nodes are part of the lymphatic system, acting to protect body fluids by filtering out and destroying bacteria and other harmful substances from lymph that is continually carried to them by lymph vessels.
Cleaned lymph is carried away from the nodes by lymph vessels to the bloodsteam where it helps forms blood plasma. Lymph nodes produce various blood cells needed to fight infection which includes lymphocytes.
Lymphocytes are small white blood cells that plays a major role in defending the body against disease. There are two types of lynphocytes: B cells, which make antibodies that attack bacteria and toxins, and T cells which attack body cells themselves when they have been taken over by viruses or become cancerous.
Lymph nodes that become enlarged doing battle with an infection or as a result of injury nearby usually resolve with treatment of the infection or injury. However, if the cause is cancer, the nodes would need to be treated as well as the cancer.
What Is Lymphadenopathy In Celiac Disease and/or Gluten Sensitivity?
[dropcap]P ruritic skin is a symptom of a primary disease that may involve only the skin or a systemic disorder with other features and is characterized by chronic itching.
Q: What part of skin is affected by itchiness?
A: Itching may arise from any layer of skin, depending on the cause.
In the image to the right, the outermost protective surface layer, or stratum cornem, is shown as a thin tan line. It is the top dead layer of the epidermis that normally sloughs off as new cells move up to replace it. The epidermis is shown as a dark pink layer. It is composed of five layers of keratinocytes that flatten as they move upward.
The pink layer under the epidermis is the dermis, or true skin, which is composed of collagen and elastin tissue. It contains oil glands that lubricate skin, sweat glands, blood vessels, nerve endings, lymphatics, and hair follicles. Under the dermis is subcutaneous tissue containing fat cells here colored yellow on the bottom of the image.
What Is Pruritic Skin In Celiac Disease and/or Gluten Sensitivity?
[dropcap]S eborrhea dermatitis is a recurring inflammatory disorder of sebaceous glands characterized by scaly patches of skin, often with bumps.
Seborrhea dermatitis results from the body’s inflammatory reaction to invasion by pityrosporum yeast that naturally inhabits the scalp and skin.1 Inflammation is the normal response to tissue injury and germ invasion.
Pityrosporum is a yeast that is commonly present worldwide. Its development depends on various factors that predispose to pityriasis versicolor, a chronic and mild superficial yeast infection. These infections usually are asymptomatic without itching or pain and without cellular and/or antibody responses.2
Q: Why are the sebaceous glands particularly affected by this yeast?
A: Pityrosporum yeast is an organism that needs oil produced by sebaceous glands to grow. If conditions permit, this yeast invades the superficial layer of skin and hair shafts to reproduce, causing infection. Such conditions include weakened skin due to nutritional deficiencies, excessive build-up of oil on skin, and altered immunity due to systemic disease such as psoriasis.
In adults, areas of skin that are the most affected have the greatest number of sebaceous glands especially the scalp, back, underarms, and the face including the eyelids, eyebrows and side folds of the nose.
All ages are subject to seborrhea dermatitis, and males have a higher occurence than females.
What Is Seborrhea In Celiac Disease and/or Gluten Sensitivity?
Zarei-Mahmoudabadi A, Zarrin. M, Mehdinezhad F. Seborrheic dermatitis due to Malassezia species in Ahvaz, Iran. Iran J Microbiol. 2013 Sep;5(3):268-71. [↩]
What Is Vitiligo? [dropcap]V itiligo is a pigmentation disorder of the skin characterized by permanent loss of melanocytes in defined areas and, in some patients, antibodies to melanin. Vitiligo has significant psychological impact if occurring before…
Mucosa in refractory celiac disease immunostained sequentially for CD3 (alkaline phosphatase-blue) and CD8 (peroxidase-brown). Most intraepithelial lymphocytes are CD3+, CD8-. Courtesy pubcan.org
What Is Refractory Celiac Disease?
[dropcap]R efractory celiac disease, formerly called refractory sprue, is a severe complication characterized by persistence of symptoms and intestinal inflammation despite gluten free diet after 12 months.1
Refractory celiac disease appears in two forms, ulcerative jejunitis (RCD I) and cryptic intestinal T-cell lymphoma (RCD II).
Patients with RCD I seem to profit from immunosuppressive treatment, but positive response to corticosteroid treatment does not exclude underlying enteropathy–associated T-cell lymphoma (EATL).
Patients with RCD II have a high percentage of abberant T-cells and is usually resistant to medical therapies. The presence of an aberrant clonal intraepithelial T-cell population has led to the designation of refractory celiac disease with this population as a cryptic intestinal T-cell lymphoma, characterized by frequent dissemination to the blood and the entire gastrointestinal lining.2
Refractory sprue may occur after an initial response to gluten free diet or without any evidence of preexisting celiac disease. All other causes of malabsorption must be excluded, such as collagenous colitis.
In a subgroup of patients with enteropathy-associated T-cell lymphoma (EATL) there is progressive deterioration of a refractory form of celiac disease. The prognosis is poor, although some patients respond to corticosteroids and immunosuppressive agents.3
A nationwide Finnish study showed that patients of male gender, older age, severe symptoms or seronegativity (negative antibody result) at the diagnosis of celiac disease are at risk of future refractory coeliac disease and should be followed up carefully.4
Chorea has been described as a paraneoplastic phenomenon in patients with non-Hodgkin’s lymphoma and has been described as associated with lymphoma arising from a background of refractory celiac disease. The finding of chorea in association with celiac disease should prompt a search for possible underlying intestinal T-cell lymphoma.5
How Prevalent Is Refractory Celiac Disease?
Sources:
Murray JA, The widening spectrum of celiac disease. American Journal of Clinical Nutrition. Mar 1999;69 (3):354-365. [↩]
Culliford AN, Green PH. Refractory sprue. Current Gastroenterology Reports. Oct 2003;5(5):373-8. [↩]
Culliford AN, Green PH. Refractory sprue. Current Gastroenterology Reports. Oct 2003;5(5):373-8. [↩]
Ilus T, Kaukinen K, Virta LJ, Huhtala H, Mäki M, Kurppa K, Heikkinen M, Heikura M, Hirsi E, Jantunen K, Moilanen V, Nielsen C, Puhto M, Pölkki H, Vihriälä I, Collin P. Refractory coeliac disease in a country with a high prevalence of clinically-diagnosed coeliac disease. Aliment Pharmacol Ther. 2014 Feb;39(4):418-25. doi: 10.1111/apt.12606. [↩]
Kitiyakara T, Jackson M, Gorard DA. Refractory coeliac disease, small-bowel lymphoma and chorea. J R Soc Med. 2002 Mar;95(3):133-4. [↩]
Drawing of Biopsy Showing Muscle Fibers Invaded by Immune Cells. Courtesy MDA.org
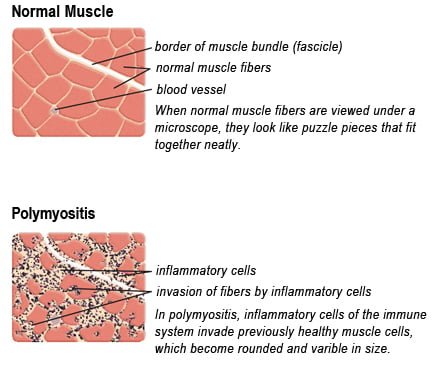
What Is Polymyositis?
[dropcap]P olymyositis is a body-wide connective tissue disease resulting from autoimmune attack of skeletal muscles that is characterized by inflammatory and degeneratory changes. The course is unpredictable being marked by spontaneous flare-ups and remissions.
Polymyositis can begin slowly or abruptly according to the factor that is triggering the onset such as infection, medications like phenytoin, and autoimmune disease.
Progressive muscle weakness starts in the proximal skeletal muscles (muscles closest to the trunk of the body).
Skeletal muscles, also called voluntary, are muscles that move the body as we want, such as walking and lifting objects, as opposed to those we cannot voluntarily control, such as the muscles of digestion.
Q: What are the degeneratory changes in skeletal muscles?
A: In polymyositis, degeneratory changes in skeletal muscles means that muscles are being destroyed (called necrosis), resulting in fibrosis, or scarring. When scar tissue takes the place of lost muscle tissue, it cannot act like muscle to contract and relax. Muscle destruction is what causes muscle pain and weakness.
After the clinical work-up of exams and blood studies to determine muscle damage, the diagnosis of polymyositis is confirmed by muscle biopsy. See image at above left. The black dots are inflammatory cells. Edema (fluid) between cells caused by inflammation pushes muscle fibers apart.
There is no cure for polymyositis, but the symptoms can be treated. Options include medication, physical therapy, exercise, heat therapy (including microwave and ultrasound), orthotics and assistive devices, and rest. The standard treatment for polymyositis is a corticosteroid drug, given either in pill form or intravenously. Immunosuppressant drugs, such as azathioprine and methotrexate, may reduce inflammation in people who do not respond well to prednisone.
Periodic treatment using intravenous immunoglobulin can also improve recovery. Other immunosuppressive agents used to treat the inflammation associated with polymyositis include cyclosporine A, cyclophosphamide, and tacrolimus. Physical therapy is usually recommended to prevent muscle atrophy and to regain muscle strength and range of motion.1
Diagnosis is based on elevated muscles enzymes, increased urinary creatine level, and electromyograph abnormalities.
Polymyositis can affect people at any age. It is most common in adults between ages 50 and 70, and in children ages 5 to 15. It affects women twice as often as men and is more common in African Americans than Caucasians.2 The major causes of death from polymyositis are cancer and lung disease, including pneumonia. The 5-year mortality rate can be as high as 1 in 5 patients.2
What Is Polymyositis In Celiac Disease and/or Gluten Sensitivity?
Sources:
National Institute of Neurological Disorders and Stroke [↩]
 What Are Extraintestinal Lymphomas?
What Are Extraintestinal Lymphomas?