
Contents
What Is Dermatitis Herpetiformis?
[dropcap]D[/dropcap]ermatitis herpetiformis (DH) is an autoimmune extremely itchy, painful bullous skin rash (blistering eruptions) arising from the underlying dermis layer of skin as a consequence of gluten sensitivity.
Dermatitis herpetiformis is characterized by multiple intensely itchy, red blisters appearing on the elbows which can extend down the forearm to the wrist and the knees. Less usual areas involve the back, buttocks, scalp, and abdomen.
Q: Do the blisters leave a mark when healed?
A: Crops of skin eruptions begin with itching or a burning sensation in reddened papules. There are grouped vesicles and tense blisters. The blister contents may be serous or bloody, with symmetrical distribution (eg, both knees or both elbows). Fluid filled elements rupture leaving denuded areas of sore skin and crust. Subsequently, there is residual hypopigmentation (a white area) or hyperpigmentation (dark area).1
Rupture of blisters begins relief from intense burning and itching.

What Is Dermatitis Herpetiformis In Celiac Disease and/or Gluten Sensitivity?
Primary care providers should be aware of this skin condition, as they are more likely than a gastroenterologist to be confronted with this type of presentation of celiac disease.2
-
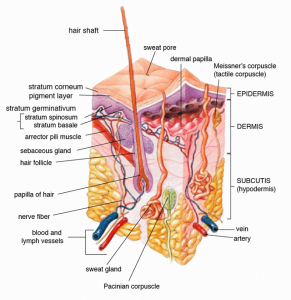
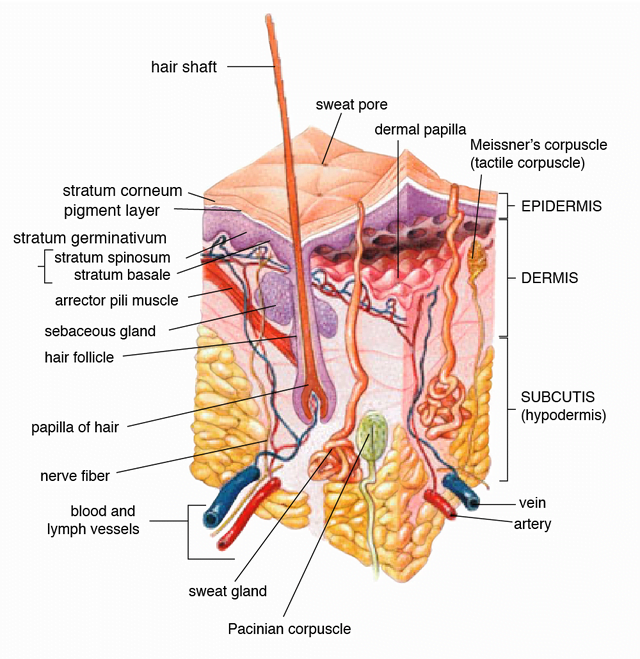
Diagram of Skin Structure. Wikipedia. Relationship between dermatitis herpetiformis and celiac disease. Dermatitis herpetiformis is a cutaneous (skin) manifestation of celiac disease developing in those patients with mild celiac disease who produce epidermal (skin) transglutaminase autoantibodies (tTG) of high avidity (strength of binding site) and affinity (strength of antigen-antibody complex formed) for skin. The main function of tTG in the epidermis is to save the integrity of the skin.3
- Relationship between dermatitis herpetiformis and IgA deposits. Serum IgA in dermatitis herpetiformis binds epidermal transglutaminase,4 causing IgA to clump and form deposits of this antibody in the papillary dermis (deeper level of skin).
- Relationship between dermatitis herpetiformis and circulating blood antibodies. Despite forming IgA deposits in their skin, patients with dermatitis herpetiformis have no circulating autoantibodies (in their blood) binding to the cutaneous basement membrane components or to other adherent structures of the skin, even considering that epidermal transglutaminase (TGase 3) is the autoantigen of dermatitis herpetiformis.5 However, 40% of dermatitis herpetiformis patients do have IgA-containing circulating immune complexes not binding skin.6
- Relationship between dermatitis herpetiformis and antibody tests showing intestinal damage. Because dermatitis herpetiformis presents variable degrees of enteropathy, the correlation with blood antibody tests is difficult. The tests indicated are IgA antiendomysial (EMA) and/or anti-tissue transglutaminase. (tTG). Both correlate with small bowel damage and adherence to gluten-free diet. Sugai et al. suggested that deamidated synthetic gliadin-derived peptide (a-GDP) was more sensitive.5
- Relationship between dermatitis herpetiformis and intestinal damage. The damage to the small intestine may be asymptomatic when the skin rash appears, but is indistinguishable from that seen in celiac disease.7 The prevalence of villous atrophy was significantly higher in the patients who presented with celiac disease than in those who presented with dermatitis herpetiformis alone (61.8 vs. 12.5%).8
- Relationship between dermatitis herpetiformis and nutritional deficiencies. The prevalence of nutritional deficiencies occurred at a similar rate in patients with dermatitis herpetiformis and patients with celiac disease without dermatitis herpetiformis.8
- Relationship between dermatitis herpetiformis and bone loss. Bone mineral content in patients with dermatitis herpetiformis is significantly lower than in healthy controls, but higher than in celiac disease. Bone mineral content in patients with dermatitis herpetiformis is significantly lower in those parts of the skeleton which contain more trabecular bone (lumbar spine) similar to celiac disease. However, the density of bones consisting of dominantly cortical compartment (femoral neck) did not differ in dermatitis herpetiformis (DH) and healthy subjects.3
- Relationship between dermatitis herpetiformis and inheritance. Both conditions can appear in the same family and are closely linked to HLA class 11 locus in chromosome 6. Ninety percent (90%) of patients with dermatitis herpetiformis have the genetic marker HLA DQ2 and almost all the remainder have HLA DQ8.9 Patients without the two predisposing HLA types are extremely rare.5
- Relationship between dermatitis herpetiformis and leaky gut. Intestinal permeability (leakiness), which is abnormal in all patients, and zonulin up-regulation are common and concomitant findings among patients with dermatitis herpetiformis, likely involved in pathogenesis. Patients with more severe enteropathy (damage to small intestinal lining) had significantly greater permeability. Increased permeability can be observed even in patients with no evidence of histologic damage in biopsy specimens.10
- Relationship between dermatitis herpetiformis and treatment. Oral dapsone is usually needed in patients with newly detected dermatitis herpetiformis in order to alleviate extremely itchy symptoms.11
- Relationship between dermatitis herpetiformis and fibrinolysis (normal clot breakdown or clot busting). Significantly thicker fibrin fibers were observed in clot formations of untreated, TG3 antibody positive DH patients compared to healthy controls, as well as, a significantly prolonged clot lysis time.12Prolonged clot lysis time means that the mechanism responsible for breaking down the fibrin protein framework of a clot, called fibrinolysis, is abnormal. Dapsone has a positive effect on normalizing this clot busting mechanism both before and after treatment with a gluten free diet, wherein the fiber diameters of dapsone-treated patients were similar or thinner than the control values.12
- Relationship between dermatitis herpetiformis and autoimmunity. Other associated autoimmune diseases can develop after treatment for dermatitis herpetiformis or precede it. High association autoimmune diseases include thyroid (5-11%) , pernicious anemia (1-3%), type 1 diabetes (1-2%), and collagen tissue disease.13
- Relationship between dermatitis herpetiformis and lymphoma risk. Patients with dermatitis herpetiformis can develop both B- and T-cell lymphoma as a complication.8 Researchers found that the patients with dermatitis herpetiformis who developed lymphoma (1%) had not adhered as strictly to the gluten free diet as had the control patients without lymphoma. The occurrence of lymphoma in the first-degree relatives was lower (0.2%) than in the patients with dermatitis herpetiformis.14
How Prevalent Is Dermatitis Herpetiformis In Celiac Disease and/or Gluten Sensitivity?
In a genome study involving 1550 celiac disease cases, 59 (3.8%) were positive for dermatitis herpetiformis.15
In Italy, a single referral center found that the prevalence of dermatitis herpetiformis was 4% in 770 patients diagnosed with celiac disease from January 1998 to December 2012.16
In India, dermatitis herpetiformis was found in 3.1% of children with celiac disease.17
What Are The Symptoms Of Dermatitis Herpetiformis?
Dermatitis herpetiformis is marked by the following symptoms:
- An extremely itchy and burning rash that develops into fluid filled blisters and red raised bumps on the elbows extending down lower arms on the side opposite the thumb, on the knees extending down the lower leg, trunk, and scalp.
- Rash can appear on other surfaces including the face, scalp, and hands.
How Does Dermatitis Herpetiformis Develop In Celiac Disease and/or Gluten Sensitivity?
-
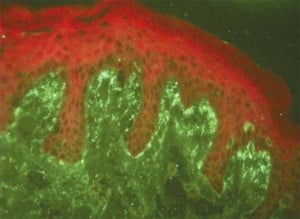
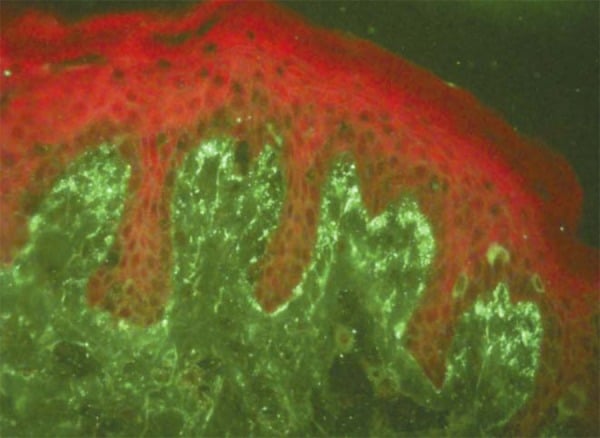
Fluorescence in Granular Pattern in the Basement Membrane Zone. Courtesy
Review: dermatitis herpetiformis
An Bras Dermatol. 2013 August;88(4):594-599.Dermatitis herpetiformis results from an etiology not fully understood involving exposure to gluten and subsequent deposition of IgA (immunoglobulin A) in the papillary dermis (deeper level of skin).18.
- An immune complex basis is most likely.19
- Increased intestinal permeability (abnormal in all patients) and zonulin up-regulation are common and concomitant findings among patients with dermatitis herpetiformis, likely involved in pathogenesis.10
Does Dermatitis Herpetiformis Respond To Gluten-Free Diet?
Yes. Dermatitis herpetiformis responds to a gluten free diet.
6 Steps To Improve Dermatitis Herpetiformis In Celiac Disease and/or Gluten Sensitivity:
- [dropcap]1[/dropcap]Remove the Trigger. Maintain a Strict, Nutritious Gluten Free Diet:
[box type=”shadow” ]Treatment. This condition responds to the complete elimination of gluten, which is the required treatment that improves both dermatitis herpetiformis and gut health.
- Gut health is the foundation to restore ALL health. Restored health will enable you to maintain a strict gluten free diet, just as other life tasks will be easier.
- A strict gluten free diet means removing 100% of wheat, barley, rye and oats from the diet.
- Cutting out bread and other obvious sources of gluten is not good enough for recovery. Even 1/8th teaspoon of flour or bread crumb is enough to sustain the inflammation that is damaging your small intestine, causing increased permeability (leaky gut) and allowing undigested gluten to enter your body where it can damage structures and function, and instigate immune inflammatory responses.
Correct Your Individual Nutritional Needs.
- Eat foods that can replenish missing nutrients. Find them under NUTRIENT DEFICIENCIES.
- Take nutritional supplements as needed. Find them under NUTRIENT DEFICIENCIES.
Recovery. You should begin to feel better within a week and notice more energy as inflammation subsides and the absorbing cells that make up the surface lining of your small intestine are better able to function.
- Intestinal lining cells are replaced every 5 days. The healing process is like sunburn where the damaged surface layer of skin sloughs off and is replaced with new normal cells.
- Leaky gut normally resolves in two month after starting a gluten free diet and brings about a big improvement in health. Improvement in intestinal permeability precedes morphometric recovery (cell appearance and structure) of the small intestine in celiac disease.20
- The intestinal lining may take up to a year to heal.[/box]
- [dropcap]2[/dropcap] Reduce Inflammation. Foods to Eat and Foods Not to Eat:
Because gluten is inflammatory, eliminate OTHER inflammatory foods from your diet to reduce an additive effect to gluten. At the same time, try to eat foods that reduce inflammation (anti-inflammatory).
[box type=”shadow” ]Here Are Major Inflammatory Food Types That Reduce Healing:
- Damaging Foods. In susceptible persons, includes corn, dairy (cow), and soy. Lactose, the sugar in any animal milk disrupts intestinal permeability causing leaky gut.21
- Allergenic Foods. Includes foods that trigger the immune sytem to produce IgE antibodies. Allergy testing is the usual way to discover these offending foods.
- Shelf Stable Processed Foods. Includes any that contain additives and preservatives. Look for them on the nutrition label of the box or package. Additives and preservatives also disrupt intestinal permeability causing leaky gut.21
- Fats. Limit deep fried foods, trans-fats, saturated fats (animal fat/butter), and EXCESSIVE omega-6 fatty acid oils like corn oil. Rancid fats, sodium caprate (a medium chain fat), and sucrose monester fatty acid (a food grade surfactant) induce significant disruption of the intestinal barrier that causes leaky gut.21.
- Excessive Refined White Flours (bran layer removed). Includes products made from them such as cookies, bread, cakes, pies. Bran contains the vitamins and minerals that metabolize grains and slows the otherwise rapid entry of sugar from their digestion into the bloodstream. Also disrupt intestinal permeability causing leaky gut.21
- Refined Sugars. Includes white sugar, corn fructose and high fructose corn syrup.
- Certain Spices. Includes paprika and cayenne pepper which disrupt intestinal permeability causing leaky gut.21
- Alcohol and Caffeine. Disrupt intestinal permeability causing leaky gut.21[/box]
[box type=”shadow” ]Here Are Important Anti-Inflammatory Food Types to Promote Health:
- Fruits. Contain ample amounts of vitamins, minerals and phytochemicals which are naturally occuring components in plants that detoxify toxins, carcinogens (reducing the risk by 50%) and mutagens.
- Non-Starchy Vegetables. Support intestinal integrity and provide ample amounts of vitamins, minerals and phytochemicals. Includes green leafy vegetables such as lettuce and kale, also onion, broccoli, garlic, and others.
- High Quality Complex Carbohydrates. Provide vitamins, minerals, and fiber while boosting serotonin levels to help you relax and feel calm. Includes whole grains, legumes, and root vegetables such as carrots, parsnips, sweet potatoes, turnips, red beets, and others.
- Antioxidants. Protect the body from inflammatory oxidant molecules that continually occur and help us handle stress and reduce irritability. Includes vitamin C-containing foods such as lemon, grapefruit, apricot, Brussels sprouts and strawberries, and others. Also, includes vitamin E-containing foods such as nuts, seeds, avocado, olive oil, and others. Cocoa is good, too.
- Omega-3 Fatty Acids. Balance opposing omega-6 fatty acids and bad fats. Fish sources includes tuna, salmon, cod, and others. Plants sources include flax, chia seeds, canola oil, and others.
- Probiotics. Supply normal microbes needed for colon health and health of the body such as these fermented foods: yogurt, kefir, and unpasteurized apple cider vinegar.
- Prebiotics/ High Fiber Foods. Food with fiber keeps our population of colonic microbes healthy.
- Protective Herbs and Spices. See below #6 below for examples.[/box]
- [dropcap]3[/dropcap] Information Sheet You Can Take to Your Doctor or Other Health Professional:
Click here.
- [dropcap]4[/dropcap] Manage Your Medications Safely:
[box type=”shadow” ]
Certain medications used to supress dermatitis herpetiformis cause nutritional deficiencies that promote complications in celiac disease. Ask your doctor or pharmacist about this possible adverse effect if you are taking any of the drugs listed below. Do not stop prescribed medications without supervision.
This is not a complete listing.
ANTIBIOTICS disrupt intestinal permeability which complicates celiac disease.
- Dapsone depletes Vitamin K.
WEIGHT LOSS DRUGS THAT BIND FAT also interfere with absorption of some nutrients.
- Zenicol (Orlistat®) depletes Vitamin K.
CHOLESTEROL DRUGS
- Colestid® and Questran® deplete Vitamin K.
[/box]
- [dropcap]5[/dropcap]Nutritional Supplements To Help Correct Deficiencies:
[box type=”shadow” ]
The type and quantity of nutritional supplements that may be needed depend on which nutrients are deficient.
- Multivitamin/mineral combination that provides 100% once a day is useful to improve overall nutrient levels. This is a safe dose, but always check with your doctor to avoid interactions with medications.
- Vitamin K as prescribed following blood test for status.
Storage Note: Store container tightly sealed, away from heat, moisture and direct light to avoid loss of potency. That is, in a safe kitchen cabinet – not in the bathroom or on the kitchen table.[/box]
- [dropcap]6[/dropcap]Manage Natural Remedies:
[box type=”shadow” ]Hydration:
- Eight glasses of water are recommended per day unless there is a contraindication such as kidney or heart disease. The Institute of Medicine recommends approximately 2.7 liters (91 ounces) of total water, from all beverages and foods, each day for women and 3.7 liters (125 ounces) daily of total water for men.
- If you are thirsty, drink water. Add fresh, squeezed lemon to water. Lemon is anti-inflammatory, alkalizing and provides vitamin C.
- Hydration Test: Urine should be pale yellow. Fingertips should be plump, without pruning but this may not be reliable when fingers are swollen with edema. Lips should be plump, without puckering. The feeling of thirst can be unreliable.
- What is wrong with soda, coffee, tea, and alcohol? These drinks are dehydrating, increase acid, and deplete nutrients.[/box]
[box type=”shadow” ]Carminatives. The following anti-inflammatory plant sources called carminitives help heal the digestive tract. They also tone the digestive muscles which improves peristalsis, thus aiding in the expulsion of gas from the stomach and intestine to relieve digestive colic and gastric discomfort.
Carminative Food Remedies:
- Raspberry.
- Carrot is also a cleansing digestive tonic.
- Grape is also bile stimulating and a cleansing remedy for sluggish digestion and laxative.
- Redbeets also stimulate and improve digestion and are easily digested.
- Cabbage also stimulates and improves digestion and is also a liver decongestant.
- Lettuce also stimulates and improves digestion and is also an alterative, meaning it improves the function of organs involved with the digestion and excretion of waste products to bring about a gradual change.
- Potatoes are antispasmodic (due to atropine like properties) and a liver remedy.
Carminative Herb Remedies:
- Sage is also a digestive, astringent, bile stimulant and energy tonic that heals the mucosa. Drink as tea or use in cooking.
- Chamomile, lemon balm, and fennel, (as a tea) also help relieve nervous tension.
- Parsley also relieves indigestion.
- Rosemary as a tea and in cooking also is a nervous system tonic for stress and fatigue, bile stimulant, and can relieve headaches and indigestion.
- Thyme is also soothing remedy useful for stimulating digestion of rich, fatty foods.
Carminative Spice Remedies:
- Cloves are also antispasmodic.
- Nutmeg is also useful for indigestion.
- Ginger.[/box]
[box type=”shadow” ]Exercise Helps:
Exercise improves circulation and rids the body of toxins.
- Walking is aerobic exercise that reconditions the whole body to improve stamina. Read more about Exercise and Fitness.
- Weight training builds muscle. Read more about Exercise and Fitness.
- Stretching improves flexibilty. Read more about Exercise and Fitness.
Note: Exercise is important, but the amount and type of exercise undertaken depends on your health. Your first priority is to heal. [/box]
What Do Medical Research Studies Tell About Dermatitis Herpetiformis In Celiac Disease and/or Gluten Sensitivity?
RESEARCH STUDY SUMMARIES
“Decreased fibrinolytic potential and morphological changes of fibrin structure in dermatitis herpetiformis.” This study investigated the fibrinolytic potential in plasma of untreated, dapsone and or/gluten-free diet treated dermatitis herpetiformis (DH) patients as well as the effect of dapsone on the fibrinolytic profile in the body. Researchers found that the fibrinolytic potential was impaired in the plasma of untreated DH patients, whereas dapsone corrected the fibrinolytic defect. These data suggest a pathogenic role for plasma-derived factors in the development of skin symptoms and add a new aspect to the long-known beneficial, symptomatic effect of dapsone in active DH.
Plasma samples of 23 DH patients, 19 healthy subjects and 5 pemphigus vulgaris patients were investigated by a turbidimetric-clot lysis assay. Out of them 5 DH plasma samples representing different fibrinolytic parameters, and 3 healthy controls were selected for parallel fibrin clot preparation. The clot fibrin structure was examined by scanning electron microscopy (SEM), and the diameters of 900 fibrin
A significantly prolonged clot lysis time was detected in untreated DH patients. The turbidity values of DH plasma clots indicated an altered fibrin structure that was also confirmed by SEM: significantly thicker fibrin fibers were observed in untreated, TG3 antibody positive DH patients compared to healthy controls, whereas the fiber diameters of dapsone-treated patients were similar or thinner than the control values. In line with the structural changes of fibrin, the fibrinolytic profile of 5 DH patients under dapsone treatment approached the control values.12
“Dermatitis herpetiformis: clinical presentations are independent of manifestations of celiac disease.” This study investigated the prevalence of features of celiac disease in those patients who presented to their doctor for dermatitis herpetiformis with those patients in whom dermatitis herpetiformis was part of a typical celiac disease presentation. Researchers found that patients who present with celiac disease and concurrent dermatitis herpetiformis are more likely to have more severe pathology than those with predominantly dermatitis herpetiformis, although nutritional deficiencies are similar between the two groups. It is important to screen for nutritional deficiencies in patients with dermatitis herpetiformis, irrespective of the presence of typical celiac disease manifestations.
A cross-sectional study of a prospectively maintained database of 1,050 patients with celiac disease was analyzed. Only biopsy-diagnosed patients were analyzed for small bowel findings. All patients were included in the analysis of autoimmune diseases and lymphoma incidence. Small bowel biopsies were classified into mild and severe.
The prevalence of villous atrophy was significantly higher in the patients who presented with celiac disease than in those who presented with dermatitis herpetiformis alone (61.8 vs. 12.5%). However, the prevalence of nutritional deficiencies, autoimmune diseases, and lymphoma occurred at a similar rate in patients with dermatitis herpetiformis and patients with celiac disease without dermatitis herpetiformis.8
“The changing clinical profile of celiac disease: a 15-year experience (1998-2012) in an Italian referral center.” This study investigating clinical, serological and histopathological findings in a large cohort of celiacs diagnosed in a single referral center found that the prevalence of dermatitis herpetiformis is 4%.
From January 1998 to December 2012, 770 patients (599 females, median age 36 years, range 18-78 years) were diagnosed with celiac disease at a hospital in Bologna, Italy. The clinical phenotypes were classified as: 1) classical (malabsorption syndrome); 2) non-classical (extraintestinal and/or gastrointestinal symptoms other than diarrhea); 3) subclinical. Serology, duodenal histology, comorbidities, response to gluten-free diet and complications were evaluated.
Disease onset was symptomatic in 610 patients (79%), while 160 celiacs showed a subclinical phenotype. In the symptomatic group the non-classical prevailed over the classical phenotype (66% vs 34%). Diarrhea was found in 27%, while other gastrointestinal manifestations were bloating (20%), aphthous stomatitis (18%), alternating bowel habit (15%), constipation (13%) and gastroesophageal reflux disease (12%). Extraintestinal manifestations included osteopenia/osteoporosis (52%), anemia (34%), cryptogenic hypertransaminasemia (29%) and recurrent miscarriages (12%).
Positivity for IgA tissue transglutaminase antibodies was detected in 97%. Villous atrophy was found in 87%, while 13% had minor lesions consistent with potential celiac disease. A large proportion of patients showed autoimmune disorders, i.e. autoimmune thyroiditis (26.3%), dermatitis herpetiformis (4%) and diabetes mellitus type 1 (3%).16
“Does dermatitis herpetiformis result in bone loss as celiac disease does? A cross sectional study.” This study investigating bone mineral density (BMD) of celiac and dermatitis herpetiformis patients found that a low bone mass is also frequent among patients with dermatitis herpetiformis. Bone mineral content in these patients is significantly lower in those parts of the skeleton which contain more trabecular than cortical bone (lumbar spine) similar to celiac disease. The density of bones consisting of dominantly cortical compartment (femoral neck) did not differ in dermatitis herpetiformis and healthy subjects.
Patient groups: 34 celiac patients, 53 with dermatitis herpetiformis and 42 healthy controls were studied. The mean age was 38.0 +/- 12.1, 32.18 +/- 14.95, 35.33 +/- 10.41 years in celiac disease, dermatitis herpetiformis, and healthy controls, respectively. Bone mineral density of the lumbar spine, the left femoral neck and radius were measured by dual-energy X-ray absorptiometry. Low bone density, osteopenia and osteoporosis were defined as a body mass density (BMD) T-score between 0 and -1, between -1 and -2.5, and under -2.5, respectively.
At lumbar region, consisting of dominantly trabecular compartment, a decreased BMD was detected in 49 % (26) patients with dermatitis herpetiformis, 62 % ( 21) of celiac disease patients, and 29 % (12) of healthy controls, respectively. Lower BMD were measured at the lumbar region in dermatitis herpetiformis and celiac disease compared to healthy subjects (0.993 +/- 0.136 g/cm2 and 0.880 +/- 0.155 g/cm2 vs. 1.056 +/- 0.126 g/cm2).3
“Celiac disease presentation in a tertiary referral centre in India: current scenario.” This facility-based retrospective observational study compared the clinical spectrum of nondiarrheal celiac disease (NDCD) with that of diarrheal/classical celiac disease (CCD) included consecutive patients diagnosed with celiac disease (CD) (as per modified ESPGHAN criteria) from October 2009 to August 2011. A total of 381 patients were diagnosed with celiac disease during the study period. NDCD was present in 192 (51.8 %). NDCD had higher mean age at presentation (5.8 ± 2.8 years vs. 6.9 ± 2.9 years respectively) and longer duration of symptoms prior to diagnosis (2.9 ± 1.7 years vs. 3.6 ± 2.2 years) as compared to CCD. Dermatitis herpetiformis was found in 3.1% of these children.
In the NDCD group, the most frequent gastrointestinal (GI) symptoms were recurrent abdominal pain [122 (63.5 %)] and abdominal distension [102 (53.1 %)] followed by constipation [48 (25 %)], vomiting [76 (39.6 %)] and recurrent oral ulcers [89 (46.4 %)]. Vomiting and constipation were more frequently seen in NDCD as compared to CCD. Common extraintestinal manifestations in NDCD included failure to thrive [109 (56.8 %)], isolated short stature [36 (18.8 %)], persistent anemia [83 (43.2 %)] and hepatomegaly/splenomegaly or both [56 (29.2 %)].
Associated comorbidities included autoimmune thyroiditis [11 (5.7 %)], type 1 diabetes mellitus [8 (4.2 %)], bronchial asthma [23 (11.9 %)], idiopathic pulmonary hemosiderosis [4 (2.1 %)], Down’s syndrome [3 (1.6 %)], alopecia areata [6 (3.1 %)], polyarthritis [2 (1.0 %)], dermatitis herpetiformis [6 (3.1 %)] and chronic liver disease [6 (3.1 %)].17
“Lymphoma in patients with dermatitis herpetiformis and their first-degree relatives.” This study investigating the occurrence of lymphoma in a large series of patients consecutively diagnosed with dermatitis herpetiformis during 1969 to 2001 and their first degree relatives demonstrated that patients with dermatitis herpetiformis can have both B- and T-cell lymphoma. The dermatitis herpetiformis patients with lymphoma (1%) had not adhered as strictly to the Gluten Free Diet as had the control patients without lymphoma. The occurrence of lymphoma in the first-degree relatives was lower (0.2%) than in the patients with DH.22
“Permeability, zonulin production, and enteropathy in dermatitis herpetiformis.” This study investigating both intestinal permeability and serum zonulin levels in patients with DH demonstrated that increased intestinal permeability (abnormal in all patients) and zonulin up-regulation are common and concomitant findings among patients with dermatitis herpetiformis, likely involved in pathogenesis. Patients with more severe enteropathy had significantly greater permeability. Increased permeability can be observed even in patients with no evidence of histologic damage in biopsy specimens.10
“Diseases associated with dermatitis herpetiformis.” This 10 year study reveals that diseases associated with dermatitis herpetiformis include autoimmune thyroid (4.3%), IDDM (1.0%), SLE (1.3%), Sjogrens syndrome (1.0%), sarcoidosis (1.3%), and alopecia areata or vitiligo (1.6%).23
CASE REPORT SUMMARIES
“Acral purpura as leading clinical manifestation of dermatitis herpetiformis: report of two adult cases with a review of the literature.” This case report describes the investigations of 2 patients with dermatitis herpetiformis in whom finger petechiae represented the initial and leading manifestation of the disease, and the confirmed diagnosis critically relied on immunopathological studies. Therefore, besides the classic causes, clinicians should also consider dermatitis herpetiformis in the differential diagnosis of acral purpura, even in patients only presenting with discrete acral petechial lesions. [Acral means it affects the fingers and/or toes of the limbs.]24
Sources:- Mendes FB, Hissa-Elian A, de Abreu MA, Gonçalves VS. Review: dermatitis herpetiformis. An Bras Dermatol. 2013 Jul-Aug;88(4):594-9. [↩]
- Robinson BL, Davis SC, Vess J, Lebel, J. Primary care management of celiac disease. Autoimmune Disorders. Nurse Practitioner. February 2015: Vol 40 – Issue 2; 28–34. [↩]
- Lorinczy K, Juhász M, Csontos Á, Fekete B, Terjék O, Lakatos PL, Miheller P, Kocsis D, Kárpáti S, Tulassay Z, Zágoni T. Does dermatitis herpetiformis result in bone loss as coeliac disease does? A cross sectional study. Rev Esp Enferm Dig. 2013 Apr;105(4):187-93. [↩] [↩] [↩]
- Karpati S. Dermatitis herpetiformis: close to unraveling a disease. Journal of Dermatological Science. Apr 2004;34(2):83-90. [↩]
- Kotze LM. Dermatitis herpetiformis, the celiac disease of the skin! Arq Gastroenterol. 2013 Jul-Sep;50(3):231-5. doi: 10.1590/S0004-28032013000200041. [↩] [↩] [↩]
- Hall RP, Lawley TJ. Characterization of circulating and cutaneous IgA immune complexes in patients with dermatitis herpetiformis. J Immunol. 1985 Sep;135(3):1760-5. [↩]
- Murray JA, The widening spectrum of celiac disease. American Journal of Clinical Nutrition. Mar 1999;69 (3):354-365. [↩]
- Krishnareddy S1, Lewis SK, Green PH. Dermatitis herpetiformis: clinical presentations are independent of manifestations of celiac disease. Am J Clin Dermatol. 2014 Feb;15(1):51-6. doi: 10.1007/s40257-013-0051-7. [↩] [↩] [↩] [↩]
- Collin P, Reunala T. Recognition and management of the cutaneous manifestations of celiac disease: a guide for dermatologists. American Journal of Clinical Dermatology. 2003;4(1):13-20. [↩]
- Smecuol E, Sugai E, Niveloni S, et al. Permeability, zonulin production, and enteropathy in dermatitis herpetiformis. Clinical Gastroenterology and Hepatology: The Official clinical Practice Journal of the American Gastroenterological Association. Apr 2005;3(4):335-41. [↩] [↩] [↩]
- Collin P, Reunala T. Recognition and management of the cutaneous manifestations of celiac disease: a guide for dermatologists. American Journal of Clinical Dermatology. 2003;4(1):13-20. [↩]
- Görög A, Németh K, Szabó L, Mayer B, Silló P, Kolev K, Kárpáti S. Decreased fibrinolytic potential and morphological changes of fibrin structure in dermatitis herpetiformis. J Dermatol Sci. 2016 Jul 6. pii: S0923-1811(16)30151-7. doi: 10.1016/j.jdermsci.2016.07.005. [↩] [↩] [↩]
- Mendes FB1, Hissa-Elian A, de Abreu MA, Gonçalves VS. Review: dermatitis herpetiformis. An Bras Dermatol. 2013 Jul-Aug;88(4):594-9. doi: 10.1590/abd1806-4841.20131775. [↩]
- Hervonen K, Vornanen M, Kautiainen H, Collin P, Reunala T. Lymphoma in patients with dermatitis herpetiformis and their first-degree relatives. British Journal of Dermatology. Jan 2005;152(Issue 1):82,5p. [↩]
- Garner C, Ahn R, Ding YC, Steele L, Stoven S, Green PH, Fasano A, Murray JA, Neuhausen SL. Genome-wide association study of celiac disease in North America confirms FRMD4B as new celiac locus. PLoS One. 2014 Jul 7;9(7):e101428. doi: 10.1371/journal.pone.0101428. eCollection 2014. [↩]
- Volta U, Caio G, Stanghellini V, De Giorgio R. The changing clinical profile of celiac disease: a 15-year experience (1998-2012) in an Italian referral center. BMC Gastroenterol. 2014 Nov 18;14(1):194. doi: 10.1186/s12876-014-0194-x. [↩] [↩]
- Bhattacharya M, Kapoor S, Dubey AP. Celiac disease presentation in a tertiary referral centre in India: current scenario. Indian J Gastroenterol. 2013 Mar;32(2):98-102. doi: 10.1007/s12664-012-0240-y. [↩] [↩]
- Karpati S. Dermatitis herpetiformis: close to unraveling a disease. Journal of Dermatological Science. Apr 2004;34(2):83-90. [↩]
- Karpati S. Dermatitis herpetiformis: close to unraveling a disease. Journal of Dermatological Science. Apr 2004;34(2):83-90. [↩]
- Cummins AG, Thompson FM, Butler RN, et al. Improvement in intestinal permeability precedes morphometric recovery of the small intestine in coeliac disease. Clinical Science. Apr 2001;100(4):379-86. [↩]
- Farhadi A, Banan A, Fields J, Keshavarzian A. Intestinal barrier: an interface between health and disease. Journal of Gastroenterology and Hepatology. 2003;18:479-91. [↩] [↩] [↩] [↩] [↩] [↩]
- Hervonen K, Vornanen M, Kautiainen H, Collin P, Reunala T. Lymphoma in patients with dermatitis herpetiformis and their first-degree relatives. British Journal of Dermatology. Jan 2005;152(Issue 1):82,5p. [↩]
- Reunala T, Collin P. Diseases associated with dermatitis herpetiformis. British Journal of Dermatology. Mar 1997;136(3):315-8. [↩]
- Tu H, Parmentier L, Stieger M, Spanou Z, Horn M, Beltraminelli H, Borradori L. Acral purpura as leading clinical manifestation of dermatitis herpetiformis: report of two adult cases with a review of the literature. Dermatology. 2013;227(1):1-4. doi: 10.1159/000347108. [↩]